Hospitals and medical facilities are saturated with information, and yet the patient leaves the appointment unbelievably confused. The chart contains too much technical jargon; the pamphlet resembles an ancient text; and the artwork never matches the explanation the physician offers in the examination room.
This explains why medical professionals are increasingly turning to AI generators like Dreamina to generate posters to illustrate medical information in a way that the patient can truly see and understand.
Medical information stays noticeable as posters
With AI-based design, even very detailed information like treatment procedures, medication timetables, and/or healing periods can be turned into nice, readable graphics. Rather than flooding them with words, you are providing them with something that only takes one quick look at, recall, and reference later. Dreamina simplifies the entire task of creating such graphics even for non-designers.
If patient education is visually appealing and easy to comprehend, patient trust will develop. And the result of patient trust is a willingness to comply, inquire, and self-manage.
Why medical visuals now mean so much
Patients are accustomed to being shown information in visual ways. They scroll, click, and zone in on things on a daily basis, so to step into an office where they are presented with a mass of words feels almost foreign to them. These posters blend icons, graphics, and simple design to meet the already existing needs of the patients.
Good visuals can also work as a means to combat anxiety. A poster that describes what happens during a procedure can calm nerves much better than a verbal explanation that goes on for a long time. Knowing what is going to happen can be less frightening than not knowing what’s going to happen.
Thus, many health care facilities have begun to move beyond general stock art to customized graphics made by artificial intelligence that serve their needs.
Benefit one: Clearer understanding in seconds
Good patient education poster communication occurs in a split second. Instead of reading three paragraphs about a disease, patients see it.
For example, one graphic might depict:
Where an organ is located
What part is affected
How the treatment works
In creating such a layout using Dreamina, you are, in fact, installing clarity within the layout. A person lacking health literacy can still go away with a newfound understanding of their condition from just this layout alone.
Benefit two: Content that matches real care
Stock photos tend to be too generic. They rarely correspond exactly to the procedure, device, or part of the body your patient has. Also, you can represent your practice in images that reflect your work on Dreamina.
This is where its AI image editor would prove to be very useful to you. Imagine you want a particular situation, and you can create an image of it, and then work on improving it until it suits your needs. This would ensure that there are no gaps between the language your doctors know and the pictures you hang on the wall.
Benefit three: Quicker updates regarding changing information
Medical standards evolve, treatment continues to advance, and clinics introduce new services. By the time posters are mass-produced, an upgraded version would be costly to produce.
“AI design reverses this process. When a protocol changes, you just have to alter the prompt and re-render the picture, and then you’re ready with a new poster to be distributed or printed,” he added. This ensures updated patient education without the need for frequent redesign.
Benefit four: Visually welcoming, not clinical
There is still a great deal of biomedical design that feels cold and frightening. Warm colors, pleasant characters, and clean design can make a big difference in how information is received.
Additionally, many of these come equipped with a design featuring a photo enhancer to brighten, sharpen, and soften the photo’s details, producing a warm, friendly poster rather than a cold one.
Benefit five: Easier sharing across spaces
The poster created by Dreamina does not necessarily have to be posted at one place only. The same image can be used on:
Waiting room screens
Clinic websites
Patient portals
Social media posts
This ensures consistency, making it easier to reinforce messages and bringing patient education as part of the total care experience rather than something dispensed at the reception desk.
Dreamina’s health lab: Main medical facts made friendlier with visuals
Dreamina helps to integrate all of the above by allowing health professionals to easily create graphics online. There’s no need to have a design team when you can create professional-looking posters in no time. All you need are instructions and a few minutes of creativity spent with Dreamina.
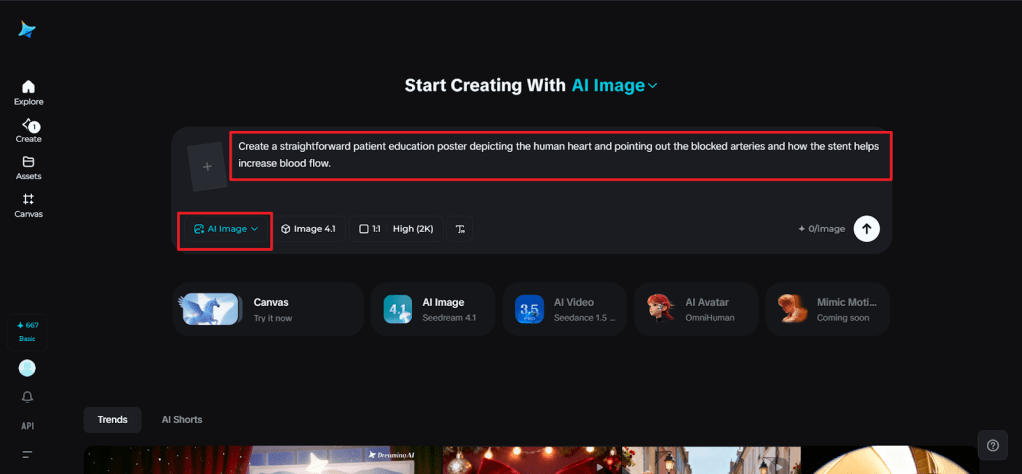
Step 1: Create the text message
Open Dreamina and log in, and go to the central creative area and concentrate on creating your patient education poster prompt. Consider writing about the subject matter and the design aesthetics.
A good example of what the prompt can be is: A straightforward patient education poster depicting the human heart and pointing out the blocked arteries and how the stent helps increase blood flow.
This kind of specificity enables Dreamina to generate an accurate and soothing visual presentation.
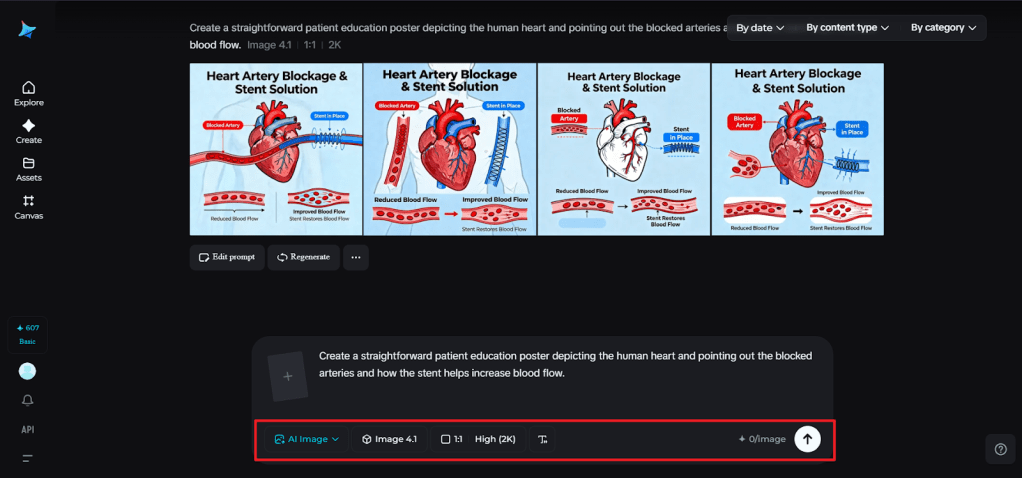
Step 2: Adjust parameters & generate
Select the model with good, precise, and clear illustrations, then set the aspect ratio based on where you intend to display the poster, whether it’s to be printed, displayed on a screen, or online. Select either 1k, which you can use for fast drafts, or 2k, which you can use for high-resolution printing. After everything is set, click on the icon of Dreamina to create your medical graphic.
Step 3: Customize and save
In Dreamina, you can use the inpaint tool to work on areas of the poster and make them clearer. Other features include expand, to give the design more space, remove, to get rid of elements that are unnecessary, and retouch, to give it a smooth look. Once you are satisfied with your poster and think it looks clear and professional, you can click on the Download icon to save and share with your patients.
Making patient education more human
When medical information is communicated visually, it turns from intimidating to empowering. Patients can point to a poster, ask questions about what they see, and remember the explanation later at home. It is that connection between image and understanding that will make AI-powered design so valuable in healthcare.
Dreamina empowers clinics and educators with a means to transform raw data into information that people can understand. It is not meant to replace medical expertise but rather supplement it by making one’s communication much clearer and even kinder.
Conclusion by feeling healthy with Dreamina
Turning medical data into patient-friendly posters isn’t just design; it’s care. When people understand their health, they make better choices and feel more confident about treatment options. In Dreamina, with just a few touches, you can create visuals that educate, reassure, and guide someone without needing a full creative team.
As healthcare continues to move toward clearer communication and patient-centered experiences, tools like Dreamina make bringing knowledge to life easier. You can help patients see their health in a whole new way with one thoughtful poster at a time.
Abdulrahman, M., Owusu, M. O., Anointed, D., Josiah, D. D., Mani, M., Muoghalu, F. E. F., & Peter, I. ode . ode . (2026). Prevalence and Determinants of Hepatitis B and C Infections among Adults in Rural Northern Nigeria: Evidence from Fufore Local Government Area Adamawa state. International Journal of Research, 13(1), 560–571. https://doi.org/10.26643/ijr/2026/27
Prevalence and Determinants of Hepatitis B and C Infections among Adults in Rural Northern Nigeria: Evidence from Fufore Local Government Area Adamawa state
Muhammad Abdulrahman1, Michael Oluyemi Owusu2, David Anointed1, Dennis Dibal Josiah3, Magaji Mani4, Fakunle Ebere Favour Muoghalu 5, Itua ode ode Peter 5
1 Faculty of Public Health Texila American University, Lot 2442, Plantation Providence, East Bank Demerara (EBD), Guyana, South America,
2Clinical Research Nurse, National Health Service (NHS), Queen Elizabeth Hospital, Mindelsohn way, Edgbaston Birmingham United Kingdom B15 2GW
3Principal Medical Officer Cottage Hospital Fufore
4Department of Nursing Science Specialist Hospital Yola, Adamawa State Nigeria.
5World Health Organization FCT Field Office, Plot 617/618 Diplomatic Drive, Central Area District, P.M.B. 2851, Garki, Abuja, Nigeria.
ABSTRACT
Background: Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections remain major public health challenges in Nigeria, particularly in rural communities with limited access to prevention and screening services. This study determined the prevalence and determinants of HBV and HCV infections among adults in Fufore Local Government Area (LGA), Adamawa State, Nigeria.
Methods: A community-based cross-sectional study was conducted among 384 adults selected using a multistage sampling technique. Data were collected using an interviewer-administered structured questionnaire, and blood samples were tested for hepatitis B surface antigen (HBsAg) and hepatitis C antibody (anti-HCV) using rapid diagnostic test kits. Descriptive statistics were used to estimate prevalence. Chi-square tests assessed associations between independent variables and hepatitis infection. Multivariable logistic regression identified independent determinants of hepatitis infection, defined as positivity to either HBsAg or anti-HCV. Statistical significance was set at p < 0.05. Determinants were analyzed using a combined hepatitis infection outcome due to overlapping transmission risk factors.
Results: The mean age of participants was 34.8 ± 10.6 years. The prevalence of hepatitis B and hepatitis C infections was 17.2% and 11.7%, respectively, while 4.7% of participants had HBV–HCV co-infection. Overall, 33.6% of respondents tested positive for at least one hepatitis infection. Independent determinants of hepatitis infection included unprotected sexual intercourse (AOR = 2.41; 95% CI: 1.31–4.45), traditional unsafe invasive procedures (AOR = 2.13; 95% CI: 1.09–4.17), sharing of sharp objects (AOR = 2.56; 95% CI: 1.30–4.70), age 35–44 years (AOR = 1.89; 95% CI: 1.02–3.49), low educational level (AOR = 2.21; 95% CI: 1.08–4.53), and marital status (AOR = 1.73; 95% CI: 1.01–3.02).
Conclusion: The prevalence of hepatitis B and C infections among adults in Fufore LGA is high, indicating sustained transmission in this rural community. Behavioral and sociodemographic factors were significant determinants, underscoring the need for targeted screening, vaccination, and community-based risk-reduction interventions.
Keywords: Hepatitis B; Hepatitis C; prevalence; determinants; rural community; Nigeria.
INTRODUCTION
Background of the Study
Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections remain major public health challenges globally, contributing substantially to liver-related morbidity and mortality. The World Health Organization (WHO) estimates that approximately 296 million people are living with chronic hepatitis B and 58 million with chronic hepatitis C worldwide, resulting in over 1.1 million deaths annually from complications such as cirrhosis and hepatocellular carcinoma (World Health Organization, 2023).
Sub-Saharan Africa bears a disproportionate share of the global hepatitis burden due to limited access to preventive services, suboptimal vaccination coverage, inadequate screening, and persistent high-risk behaviors (Olayinka et al., 2016). Nigeria is classified as a high-burden country for viral hepatitis, with a national hepatitis B prevalence estimated at approximately 8.1% and hepatitis C prevalence of about 2.2% in the general population (Tomas et al., 2021; Musa et al., 2022). However, evidence suggests that prevalence rates are often higher in rural and underserved communities, where healthcare access is limited and traditional practices involving non-sterile instruments remain common (Ndako et al., 2019).
Rural populations in northern Nigeria are particularly vulnerable to hepatitis transmission due to widespread engagement in unsafe traditional invasive procedures, sharing of sharp objects, and low awareness of transmission routes and preventive measures (Okonko et al., 2019). Anecdotal reports from local health facilities in Adamawa State indicate frequent detection of hepatitis B and C infections among adults seeking care, suggesting a potentially substantial but under-documented burden in rural communities.
Fufore Local Government Area (LGA) of Adamawa State is a predominantly rural setting characterized by farming and informal trading, with limited access to secondary and tertiary healthcare services. Despite the known risk profile of similar rural communities in northern Nigeria, there is a paucity of community-based epidemiological data on the prevalence and determinants of hepatitis B and C infections in Fufore LGA. Existing studies from Adamawa State and neighboring regions are largely facility-based or focused on specific subpopulations, limiting their generalizability to the wider adult population.
Addressing this gap is critical for informing targeted public health interventions, including hepatitis B vaccination scale-up, community-based screening, and culturally appropriate risk-reduction strategies. This study therefore assessed the prevalence and determinants of hepatitis B and C infections among adults in Fufore Local Government Area, Adamawa State, Nigeria.
Statement of the Problem
Despite global advancements in prevention and treatment, hepatitis B and C infections remain underdiagnosed, especially in rural communities in Nigeria (Musa et al., 2022). WHO identifies Nigeria as a high-burden country for HBV, with rural populations experiencing disproportionate risks due to widespread traditional invasive practices using non-sterile tools and inadequate access to healthcare services (WHO, 2023; Okwori et al., 2020).
In Fufore LGA, informal reports and field observations indicate potentially increasing prevalence of hepatitis infections among adults. High engagement in unsafe traditional invasive procedures, low awareness levels, and risky behaviors such as unprotected sex and unsafe sharing of sharp objects remain key contributors to transmission. However, there is limited local epidemiological data to guide evidence-based intervention strategies. This study therefore, determined the prevalence and determinants of hepatitis B and C infections among adults in Fufore LGA to facilitate informed public health actions for prevention and control.
Significance of the Study
This study will provide community-based evidence on the burden and determinants of hepatitis B and C infections in Fufore LGA. The findings are expected to inform public health strategies, support planning and implementation of targeted screening and vaccination programs, and guide community-based educational interventions to reduce transmission (WHO, 2023). Policymakers, healthcare providers, and stakeholders will benefit from the results in designing context-specific interventions.
Scope of the Study
The study focuses on adults aged 18 years and above residing in selected wards (Beti, Gurin, Ribadu, and Fufore) of Fufore LGA. It assesses the prevalence of hepatitis B and C infections and examines sociodemographic and behavioral determinants associated with their transmission.
Objectives of the Study
General Objective
To determine the prevalence and determinants of hepatitis B and C infections among adults in Fufore Local Government Area, Adamawa State, Nigeria.
Specific Objectives
To determine the prevalence of hepatitis B and hepatitis C infections among adults in Fufore Local Government Area.
To identify behavioral risk factors associated with hepatitis B and C infections among adults in Fufore Local Government Area.
To assess the association between selected sociodemographic characteristics and hepatitis B and C infections among adults in Fufore Local Government Area.
Research Questions
What is the prevalence of hepatitis B and hepatitis C infections among adults in Fufore Local Government Area?
Which behavioral risk factors are associated with hepatitis B and C infections among adults in Fufore Local Government Area?
What sociodemographic factors are associated with hepatitis B and C infections among adults in Fufore Local Government Area?
Research Hypotheses
Null Hypotheses (H₀)
H₀₁: There is no significant association between behavioral risk factors (unprotected sexual intercourse, sharing of sharp objects, and traditional unsafe invasive procedures) and hepatitis B and C infections among adults in Fufore Local Government Area.
H₀₂: There is no significant association between sociodemographic characteristics (age, sex, marital status, and educational level) and hepatitis B and C infections among adults in Fufore Local Government Area.
Alternative Hypotheses (H₁)
H₁₁: Behavioral risk factors (unprotected sexual intercourse, sharing of sharp objects, and traditional unsafe invasive procedures) are significantly associated with hepatitis B and C infections among adults in Fufore Local Government Area.
H₁₂: Sociodemographic characteristics (age, sex, marital status, and educational level) are significantly associated with hepatitis B and C infections among adults in Fufore Local Government Area.
Operational Definition of Terms
Burden: The prevalence of hepatitis B and C infections within the study population.
Determinants: Sociodemographic and behavioral factors contributing to hepatitis transmission.
Risk Factors: Actions or practices, such as unprotected sex, sharing sharp objects, or undergoing unsafe traditional invasive procedures, that increase the likelihood of acquiring infection.
MATERIALS & METHODS
Study design and setting
A community-based cross-sectional study was conducted in Fufore Local Government Area (LGA), Adamawa State, Nigeria. Four wards (Beti, Gurin, Fufore and Ribadu) were included. The area is predominantly rural; most residents are farmers, traders and artisans and access to secondary and tertiary health services is limited.
Study population
The study population comprised adults aged 18 years and above who had lived in the selected wards for at least six months at the time of data collection. Individuals who were critically ill or who declined to participate were excluded.
Sample size determination
The minimum sample size for prevalence studies was calculated using Cochran’s formula for proportions:
n =
Where Z = 1.96 (for 95% confidence), p = estimated prevalence, and d = desired precision (0.05).
Using the locally estimated prevalence for hepatitis B from preliminary field data (p = 0.172), the initial sample size was:
n = ≈ 218
Because a multistage cluster sampling approach was used, the sample size was adjusted for cluster design using a design effect (DEFF). A conservative design effect of 1.6was applied to account for intra-cluster correlation and the multistage procedure:
n1 = n × DEFF = 218 ×1.6 ≈349
To allow for non-response and incomplete data, a 10% contingency was added:
n = n1× (1+0.10) = 349 × 1.10 ≈384
Thus, the final sample size for the study was set at 384 participants.
Sampling procedure
A multistage sampling technique was implemented:
Ward selection (stage 1): Four wards (Beti, Gurin, Fufore and Ribadu) were purposively selected based on accessibility and local representation of the LGA.
Community selection (stage 2): Two communities were randomly selected from each of the four wards, yielding eight communities in total.
Household selection (stage 3): In each selected community, a household listing or estimate was used to calculate a systematic sampling interval. The target within-community sample was 48 participants per community (384 ÷ 8). A random start between 1 and k was chosen and every kth household was visited until 48 eligible participants were recruited.
Respondent selection (stage 4): In households with more than one eligible adult (≥18 years), one respondent was chosen by simple random selection (ballot method).
The final allocation was therefore 48 participants from each of the eight selected communities (48 × 8 = 384).
Data collection instruments and procedures
A structured interviewer-administered questionnaire was used to collect data on sociodemographic characteristics, knowledge and awareness of hepatitis, and exposure to potential risk factors (including unprotected sex, sharing of sharp instruments, and traditional invasive procedures). The questionnaire was developed in English, translated into the local languages (Hausa/Fulfulde) and back-translated to ensure accuracy.
Trained data collectors read the information sheet and consent script to prospective participants and obtained verbal informed consent prior to interview and testing. After the interview, each consenting participant underwent on-site rapid diagnostic testing for hepatitis B surface antigen (HBsAg) and hepatitis C antibody (anti-HCV) using WHO-recommended rapid test kits. Tests were performed by trained personnel following the manufacturers’ instructions and standard infection-prevention procedures (gloves, single-use lancets, safe disposal of sharps, surface disinfection). Rapid diagnostic test kits with manufacturer-reported sensitivity and specificity >99% were used.
Participants who tested positive on rapid test were counselled and provided with referral information for clinical follow-up and confirmatory testing at health facilities. All test results and responses to the questionnaire were recorded on coded study forms to protect confidentiality.
Rapid diagnostic testing results for HBsAg and anti-HCV were later recoded to generate a binary outcome variable (hepatitis infection: yes/no) for regression analysis.
Data management and analysis
Completed questionnaires and test result forms were checked daily for completeness and consistency. Data were entered into a statistical package (SPSS v26) and cleaned prior to analysis.
Descriptive analysis: Frequencies, proportions and means (± SD) were used to summarize sociodemographic variables and prevalence estimates. Prevalence of hepatitis B and hepatitis C were reported as proportions with 95% confidence intervals.
Bivariate analysis: Associations between categorical exposures (risk factors) and hepatitis serostatus were assessed using chi-square tests. Continuous variables were compared using t-tests.
Multivariable analysis: For regression analysis, hepatitis infection was defined as positivity to either hepatitis B surface antigen (HBsAg) or hepatitis C antibody (anti-HCV). Participants who tested positive for both HBsAg and anti-HCV were classified as having HBV–HCV co-infection and were included as positive cases in the combined hepatitis infection outcome. Variables with p < 0.20 in bivariate analyses were included in multivariable logistic regression models to identify independent determinants of hepatitis infection. Adjusted odds ratios (AOR) and 95% confidence intervals (CI) were reported. Statistical significance was set at p < 0.05.
Quality assurance
Data collectors underwent a two-day training covering the study objectives, questionnaire administration, informed consent procedures, rapid test performance, and infection prevention. A pilot test was carried out in a neighbouring community (not included in the main study) to refine the questionnaire and procedures. Supervisors performed daily checks on completed forms and observed testing procedures to ensure protocol adherence.
RESULT
Socio-demographic Characteristics of Respondents
A total of 384 adults participated in the study. The mean age was 34.8 ± 10.6 years (range: 18–65). Most respondents were aged 25–44 years (56.5%), female (54.4%), and married (61.2%). About48.7% had primary education, while 16.1% had no formal education.
Table 1: Socio-demographic Characteristics of Adult Respondents in Fufore Local Government Area, Adamawa State, Nigeria (n = 384)
Variable
Frequency (n)
Percentage (%)
Age (years)
18–24
77
20.1
25–34
110
28.6
35–44
107
27.9
≥45
90
23.4
Mean age ± SD
—
34.8 ± 10.6
Sex
Male
175
45.6
Female
209
54.4
Marital status
Single
78
20.3
Married
235
61.2
Divorced/Widowed
71
18.5
Education
No formal education
62
16.1
Primary
187
48.7
Secondary
89
23.2
Tertiary
46
12.0
Most respondents were within the active reproductive and economically productive age group (25–44 years), which aligns with previous studies reporting higher risk of viral hepatitis among adults due to increased exposure to behavioral risk factors (e.g., sexual activity and occupational hazards). A higher proportion of females may reflect improved healthcare-seeking behavior, similar to findings from hepatitis studies in Northern Nigeria. Lower educational attainment among nearly half of respondents may influence awareness and prevention practices relating to hepatitis. These sociodemographic patterns are consistent with findings from Gyamfi et al. (2020), who reported higher hepatitis vulnerability among adults aged 25–45 years, especially among married individuals and those with lower educational levels. Similarly, Musa et al. (2022) noted that lower education limits awareness of hepatitis prevention and contributes to increased infection risk.
Prevalence of Hepatitis B and C Infections
Of the 384 participants, 66 (17.2%) were positive for hepatitis B, 45 (11.7%) for hepatitis C, and 18 (4.7%)had co-infection.
Table 2: Prevalence of Hepatitis B, Hepatitis C, and HBV–HCV Co-infection among Adults in Fufore Local Government Area (n = 384)
Infection Status
Frequency (n)
Percentage (%)
Hepatitis B positive
66
17.2
Hepatitis C positive
45
11.7
Co-infection (HBV + HCV)
18
4.7
Negative
255
66.4
The observed HBV prevalence of 17.2% is higher than the national Nigerian average (~12%), suggesting a significant burden in this rural setting. The HCV prevalence (11.7%) is also elevated compared to sub-national reports (~7–9%), suggesting a high burden of infection in this rural community. The 4.7% co-infection rate highlights shared modes of transmission. Similar rural studies in Northeast Nigeria reported HBV prevalence between 14–18%, supporting these findings. The hepatitis B prevalence in this study (17.2%) aligns with findings by Agwale et al. (2018), who reported 16.8% among rural dwellers in Northern Nigeria. Similarly, the HCV prevalence (11.7%) is comparable to Musa et al. (2015), who found 10.5% in a related rural population. However, these figures are higher than the national estimate of HBV (8.1%) and HCV (2.2%) reported by Tomas et al. (2021), indicating a higher burden in underserved rural communities.
Distribution of Behavioral Risk Factors
Unprotected sex was the most common risk factor (59.6%), followed by unsafe traditional invasive procedures (56.5%) and sharp object sharing (50.5%).
Table 3: Distribution of Behavioral Risk Factors for Hepatitis Infection among Adults in Fufore Local Government Area (n = 384)
Risk Factor
Yes n (%)
No n (%)
Unprotected sexual intercourse
229 (59.6)
155 (40.4)
Traditional unsafe invasive procedures
217 (56.5)
167 (43.5)
Sharing sharp objects (blades/needles)
194 (50.5)
190 (49.5)
Previous blood transfusion
72 (18.8)
312 (81.2)
History of STIs
59 (15.4)
325 (84.6)
High engagement in unprotected sexual intercourse and unsafe invasive procedures contributes significantly to viral hepatitis transmission. Traditional practices involving scarification and tribal markings remain prevalent in rural communities, corroborating findings from Northern Nigeria. Sharp object sharing is common due to low access to sterile instruments. These findings are comparable to those of Okonko et al. (2019), who identified unprotected sex and sharing of sharp objects as the primary transmission routes in rural Nigerian populations. Orji et al. (2013) also emphasized the role of cultural invasive practices such as scarification in driving hepatitis transmission among communities with limited access to modern healthcare.
Association between Selected Factors and Hepatitis Infection
Bivariate analysis using the chi-square test showed statistically significant associations between hepatitis infection and marital status (χ² = 6.15, p = 0.046), unprotected sexual intercourse (χ² = 6.80, p = 0.009), exposure to traditional unsafe invasive procedures (χ² = 5.12, p = 0.024), and sharing of sharp objects (χ² = 7.05, p = 0.008). Sociodemographic variables with incomplete cross-tabulated data were not included in the chi-square analysis but were assessed in the multivariable logistic regression model.
Table 4: Bivariate Association between Selected Behavioral Factors and Hepatitis Infection among Adults in Fufore Local Government Area (n = 384)
Variable
Hepatitis Positive n (%)
Hepatitis Negative n (%)
χ²
p-value
Marital status
6.15
0.046
Married
48 (20.4)
187 (79.6)
Others (single/divorced/widowed)
18 (12.9)
131 (87.1)
Unprotected sexual intercourse
6.80
0.009
Yes
46 (20.1)
183 (79.9)
No
20 (12.9)
135 (87.1)
Traditional unsafe invasive procedures
5.12
0.024
Yes
41 (18.9)
176 (81.1)
No
25 (15.0)
142 (85.0)
Sharing sharp objects
7.05
0.008
Yes
39 (20.1)
155 (79.9)
No
27 (14.2)
163 (85.8)
Footnote: Hepatitis infection was defined as positivity to either hepatitis B surface antigen (HBsAg) or hepatitis C antibody (anti-HCV). Percentages are row percentages. Chi-square test was used to assess associations. Statistical significance was set at p < 0.05.
Multivariable Logistic Regression Analysis of Determinants of Hepatitis Infection
Because the study aimed to identify shared community-level determinants, HBV and HCV outcomes were combined into a single ‘hepatitis infection’ variable for regression analysiscdo
Table 5: Multivariable Logistic Regression Analysis of Determinants of Hepatitis Infection among Adults in Fufore Local Government Area, Adamawa State, Nigeria (n = 384)
Determinant
AOR
95% CI
p-value
Interpretation
Unprotected sex
2.41
1.31–4.45
0.005
Significant
Traditional unsafe procedures
2.13
1.09–4.17
0.028
Significant
Sharing sharp objects
2.56
1.30–4.70
0.006
Significant
Age (35–44 years)
1.89
1.02–3.49
0.041
Significant
Low education (none/primary)
2.21
1.08–4.53
0.030
Significant
Marital status (married)
1.73
1.01–3.02
0.048
Significant
Sex
1.12
0.67–1.87
0.542
Non-significant
Footnote: Hepatitis infection was defined as positivity to either hepatitis B surface antigen (HBsAg) or hepatitis C antibody (anti-HCV). Participants who tested positive for both HBsAg and anti-HCV were classified as having HBV–HCV co-infection and were included as positive cases in the regression model. AOR = Adjusted Odds Ratio; CI= Confidence Interval.
Behavioral factors (unprotected sex, sharp instrument sharing, and unsafe traditional procedures) were independently associated with a two – to three-fold higher odds of hepatitis infection. Sociodemographic determinants such as middle-age, low education, and marriage also showed independent associations. These findings mirror similar studies across Sub-Saharan Africa that emphasize both cultural and behavioral drivers of transmission. These determinants are in line with observations by Ndako et al. (2019), who identified unsafe traditional procedures and low education as independent predictors of hepatitis infection. The increased risk among married adults supports findings from Abdou et al. (2020), which linked marital sexual exposure to higher viral hepatopathy rates due to low condom usage.
DISCUSSION
This study examined the prevalence and determinants of hepatitis B and C infections among adults in Fufore Local Government Area, Adamawa State, Nigeria. The findings demonstrate a substantial burden of hepatitis infection in this rural population, reinforcing concerns that viral hepatitis remains an under-recognized public health problem in underserved communities with limited access to preventive and screening services.
Bivariate Associations
Bivariate analysis using the chi-square test revealed significant associations between hepatitis infection and selected behavioral factors, including marital status, unprotected sexual intercourse, exposure to traditional unsafe invasive procedures, and sharing of sharp objects. These associations highlight the importance of behavioral and cultural practices in shaping hepatitis transmission dynamics in rural settings. Similar findings have been reported in previous Nigerian and sub-Saharan African studies, where unsafe sexual practices and informal invasive procedures contribute significantly to hepatitis transmission.
The observed association with marital status may reflect differences in sexual behavior patterns and cumulative exposure risks; however, this finding should be interpreted cautiously, as marital status may serve as a proxy for other unmeasured behavioral or social factors. Overall, the bivariate findings suggest sustained community transmission driven largely by preventable behavioral exposures.
Multivariable Analysis
Multivariable logistic regression identified independent predictors of hepatitis infection after adjusting for potential confounders. The persistence of behavioral risk factors as significant predictors in the adjusted model underscores their central role in ongoing hepatitis transmission within the study population. Unlike bivariate analysis, the regression model allowed for simultaneous assessment of sociodemographic and behavioral variables, providing a more robust understanding of factors independently associated with hepatitis infection.
Sociodemographic variables, including age and education level, were assessed in the regression model despite not being included in the chi-square analysis due to incomplete cross-tabulated data. Their inclusion in the multivariable analysis strengthens the validity of the findings by accounting for confounding influences that may not be evident in unadjusted comparisons.
Hepatitis B Virus (HBV)
The burden of hepatitis B infection observed in this study has important public health implications, particularly given the availability of an effective vaccine. The findings suggest gaps in hepatitis B vaccination coverage among adults in rural communities, where routine screening and catch-up vaccination programs are often limited. Continued exposure to unsafe sexual practices and invasive cultural procedures further increases the risk of HBV transmission. Strengthening hepatitis B vaccination strategies, including adult catch-up vaccination and improved access to screening services, is critical to reducing HBV-related morbidity in rural populations.
Hepatitis C Virus (HCV)
Hepatitis C infection, which lacks a preventive vaccine, was also prevalent among study participants and was closely linked to blood-borne risk behaviors such as sharing sharp objects and exposure to unsafe traditional procedures. These findings are consistent with the known transmission pathways of HCV and emphasize the need for enhanced screening and early detection strategies. Integrating routine HCV screening into primary healthcare services, particularly in rural and high-risk communities, is essential for timely diagnosis and linkage to care.
Public Health Implications
Overall, the findings suggest sustained community transmission of viral hepatitis in Fufore LGA, driven largely by modifiable behavioral and cultural practices. Targeted community-based health education, regulation of traditional invasive practices, expansion of hepatitis B vaccination coverage, and improved access to hepatitis C screening are critical interventions for reducing the burden of viral hepatitis in rural Nigerian communities.
CONCLUSION
This study demonstrates a high burden of hepatitis B and C infections among adults in rural Fufore Local Government Area, with infection strongly associated with behavioral and cultural risk practices. The findings highlight persistent gaps in hepatitis prevention services, particularly hepatitis B vaccination coverage and access to hepatitis C screening. Addressing unsafe traditional practices, strengthening behavioral risk reduction interventions, and scaling up hepatitis prevention and screening programs are urgently needed to reduce the burden of viral hepatitis in rural Nigeria.
Authors’ Contributions
Muhammad Abdulrahman conceived and designed the study, analyzed the data, and drafted the manuscript. Michael Oluyemi Owusu contributed to study design and critically reviewed the manuscript. David Anointed and Dennis Dibal Josiah supported data collection and field supervision. Magaji Mani provided technical public health input. Muoghalu Ebere Favour and Itua Ode Ode Peter contributed to data interpretation and manuscript revision. All authors reviewed and approved the final manuscript and accept responsibility for its content.
Conflict of Interest:The authors declare that they have no competing interests.
Source of Funding: None
REFERENCES
Abdou, R., Hassane, M., Moussa, A., & Oumarou, H. (2020). Sexual behaviour, marital status and risk of viral hepatitis infection among adults in Sub-Saharan Africa. African Journal of Reproductive Health, 24(3), 102–111.
Agwale, S. M., Tanimoto, L., Womack, C., & Watanabe, K. (2018). Prevalence of hepatitis B virus infection among rural populations in Northern Nigeria. Journal of Viral Hepatitis, 25(7), 785–792.
Gyamfi, C., Agyeman, A. A., & Frempong, M. T. (2020). Sociodemographic determinants of viral hepatitis infection among adults in rural West Africa. BMC Public Health, 20(1), 1458–1466.
Musa, B. M., Bussell, S., Borodo, M. M., Samaila, A. A., & Femi, O. L. (2015). Prevalence of hepatitis C virus infection in Nigeria, 2000–2013: A systematic review and meta-analysis. Nigerian Journal of Clinical Practice, 18(2), 163–172.
Musa, B. M., Zubair, S. A., Samaila, A. A., & Borodo, M. M. (2022). Epidemiology of viral hepatitis in Nigeria: Burden, transmission dynamics and public health implications. Annals of African Medicine, 21(1), 1–9.
Ndako, J. A., Onwuliri, E. A., & Agabi, Y. A. (2019). Risk factors associated with hepatitis B and C infections in rural Nigerian communities. Journal of Community Health, 44(4), 785–793.
Okonko, I. O., Okerentugba, P. O., & Akinpelu, A. O. (2019). Transmission dynamics of hepatitis B and C viruses in rural Nigerian settings. African Health Sciences, 19(1), 1839–1848.
Okwori, A. E. J., Sadiq, M. N., & Ngwai, Y. B. (2020). Traditional practices and the risk of blood-borne viral infections in rural Nigeria. Nigerian Medical Journal, 61(2), 67–74.
Olayinka, A. T., Oyemakinde, A., Balogun, M. S., Ajudua, A., Nguku, P., Aderinola, M., & Nasidi, A. (2016). Seroprevalence of hepatitis B infection in Nigeria: A national survey. The American Journal of Tropical Medicine and Hygiene, 95(4), 902–907.
Orji, M. O., Mba, N. C., & Ogbu, O. (2013). Cultural practices and risk of viral hepatitis transmission in rural African populations. Journal of Infection in Developing Countries, 7(6), 455–461.
Tomas, J., Adekanle, O., & Adebayo, S. (2021). National prevalence of hepatitis B and C infections in Nigeria: A systematic review. Pan African Medical Journal, 38, 132–141.
World Health Organization. (2023). Global hepatitis report 2023. World Health Organization.
“Quality Education” the fourth goal among the seventeen Sustainable Development Goals (SDG) outlined by the United Nations, is “to ensure inclusive and equitable quality education and promote lifelong learning opportunities for all”. These descriptions are remarkably similar to the focus identified through this research and, with this in mind, the three dimensions of this research are further explained as being; (1) the ‘Importance of Interaction’ – referring to the various levels of interaction between individuals within the school environment, accounting for behaviour, atmosphere, and types of communication, (2) the ‘Dynamics of Individuation’ – referring to the way in which the differing needs of individuals are personalised and catered for, accounting for classroom pedagogical approaches and student diversification, and (3) the ‘Need for Psychological Support’ – referring to the way in which individuals within the school and the school as a whole is supported by its community, from both an educational and psychological perspective. By suggesting that these research directions are intertwined concepts, they propose a holistic observation of contributing factors that influence the educational process.
This assessment could be used to identify teacher strengths from a personal, interpersonal, psychological, and pedagogical perspective. The Questionnaire of Teacher Interaction (QTI), Technological Pedagogical and Content Knowledge (TPaCK), and Mental Health Inventory (MHI) were used in the pilot study and were considered to be suitable for the needs of this research stage.
The ‘Educational Bubble’
In a recent talk, Seema Bansal (2016) mentioned being asked by the then head of the Department of Education in the state of Haryana (India), for help in addressing issues in their public schools. These ‘issues’ ranged in detail and complexity, including that up to 50% of students fall so far behind their peers before the age of eleven that they will be unable to recover. Despite public schools offering free meals or books to students, it was also found that 40% of parents would pull their children out of these public schools and register them into private schools. Bansal (2016), representing BCG (Boston Consulting Group), was asked to assist in the education renovation of an Indian state of Haryana, which consists of 15,000 public schools with over 2 million students. Bansal mentions needing to uncover the factors that have caused the educational issues in the first place and, in identifying the goals necessary to develop strategies for reaching this particular goal, decided to go directly into classrooms and observe the way educators were teaching. Reporting that the problem within Indian schools was the quality of education, not access to education, mentions that Bansals’ BCG team devised a three-year plan that was based around student learning outcomes and explicit focusing of accountability, data systems, and organizational capacity.
Bansal (2016) reports that Haryana teachers were very capable of teaching a class but, the majority of their time was spent outside of the classroom; this was interesting as, before physically entering a classroom, non-educators had apparently viewed teachers being ‘lazy’ or ‘incapable’. Although Bansal (2016) reported teachers not necessarily teaching, she mentions that it was because they were supervising the construction of new classroom buildings, supervising the cooking of student lunches, or visiting a bank to deposit scholarship money for students. This particular insight was (and is) incredible; Bansal asked teachers why they were not teaching and the teachers answered by saying that “when a supervisor comes to visit us, these are exactly the things that he checks” (5:29). This particular finding shows that in the provision of government programmes in Haryana, designed to motivate students to stay in school and give greater access, had become an additional point of accountability for teachers and had started to impede classroom instruction. Seeing this as an issue, Bansal and her team began to look at the literature at various educational programmes and pilot programmes that have been shown to improve instructional practice. However, what a large proportion of individuals fail to recognise is how the implementation of these programmes will always come at a cost. For example, schools that take part in a pilot that explores the use of innovative technologies on student learning might show that this programme does indeed result in higher levels of academic outcomes.
In Bansal’s (2016) talk she mentions that, with regards to studies and interventions, researchers will typically bring in resources such as money, experience, research assistants, or products. Unless researchers intend to roll out this innovation across every classroom in the country, the findings are most likely going to be un-scalable, ungeneralisable, unusable, and does not reflect a real-world classroom setting. It has been previously mentioned that “teaching requires being responsive to real-world conditions and constraints that shape the activities of the classroom and students” (Motoca et al., 2014, pg. 120). This view is similar to schools being ‘learning organisations’ where the “emphasis of research might be more upon the selection and differentiation of pupils and on their subculture rather than on the authority structure or the decision-making processes within the school” (Bell, 1980, pg.183). Hamzah, Yakop, Nordin and Rahman (2011) explain that, like all organisations, there is a strong emphasis on schools to adapt to their surroundings, encourage flexibility, and to be responsive to the various societal and cultural changes across an educational landscape.
While there is a large body of evidence favouring schools as learning organisations (Mulford, 1997; Stoll and Fink, 1996), research concerning how a school should go about this change is not as prevailing (Silins, Zarins, & Mulford, 2002). While it is clear that there are similarities between a school and an ‘organisation’, both have structure, both have management, there is leadership, interaction, and varying levels of accountability, it is also clear that many factors influence the way in which both operate. Johnston (1998) sought to investigate the key characteristics that involved a school identifying itself as being a ‘learning organisation’. Although focusing exclusively on post-primary schools based in Austrailia, it was found that inclusive, collaborative structures, effective communication channels, integrated professional development, and learning-focused leadership were the four main characteristics of schools being one of these ‘learning organisations’.
Under the three guiding topics of this research, explicitly outlined through questions and hypotheses, this current research sought to discover what the Irish educational environment needs and how a piece of research could be used practically to support school systems and the individuals within them. This research is looking towards the perception of a school being a learning organisation; considering the way which Silins, Zarins and Mulford’s (2002) express the four factors of ‘learning organisations’ above. These descriptions are remarkably similar to the focus identified through this research and, with this in mind, the three dimensions of this research are further explained as being; (1) the ‘Importance of Interaction’ – referring to the various levels of interaction between individuals within the school environment, accounting for behaviour, atmosphere, and types of communication, (2) the ‘Dynamics of Individuation’ – referring to the way in which the differing needs of individuals are personalised and catered for, accounting for classroom pedagogical approaches and student diversification, and (3) the ‘Need for Psychological Support’ – referring to the way in which individuals within the school and the school as a whole is supported by its community, from both an educational and psychological perspective. By suggesting that these research directions are intertwined concepts, they propose a holistic observation of contributing factors that influence the educational process.
While research in an Irish context has found that only 33.1% of schools regularly engage with SSE (Brown, 2010), this dispute between the DES and teaching unions will cause frustration, anxiety, and confusion throughout the educational community. The SSE is a thorough research process that requires considerable resources, the problem is one of ‘lack of support’, almost mirroring the issues faced by Bansal’s (2016) team in Haryana. Additionally, this lack of support echoes in other ways. For example, on 30th of March 2016, the INTO released a press release that argued against the cut in government funding for education and highlighted that schools are being forced to fundraise themselves, that they are “kept running on cake sales, raffles and sponsored walks” (2016b), despite having no empirical evidence to support.
3.6. Conclusion – The Individualised Teacher Report
This claim within the press release itself, it does clearly articulate the many problems experienced in Irish Education.
Despite focusing on the individual educator, rather than the collective school environment, this Ph.D. project somewhat resembles the development of a self-evaluation process; it requires educators to compete measures that evaluate their subjective instructional and psychological resources. Although the issues surrounding self-evaluation may be a possible limitation, this research would argue the opposite. This study could provide a process that allows schools to self-evaluate in a way that takes the workload away from schools, provides tailored feedback to individual educators, has a standardised methodological approach, and is evidence based and research driven. A new model of self-evaluation may be considered a momentous task; however, it is not beyond the scope of this project.
According to Collins and Pratt (2011), “there is a move to adopt a single, dominant view of effective teaching … [where] teachers are asked to reflect on who they are and how they teach but with an implied message that reflection should conform to some preconceived notion of a ‘good’ teacher” (pg. 359). It is naïve to assume that there is a ‘single view’ of what it means to be an effective educator, as the requirements and needs of one classroom group will differ that than of another. What is arguably more appropriate for education, rather than training educators to teach in the same way and conform to a preconceived notion of what a ‘good teacher’ is, is to encourage and train teachers to be self-reflective and adapt their teaching to suit the needs of their students. Boud, Keogh, and Walker (1985) mentioned that reflective practice is an important human activity where provision is given for individuals to recapture their experiences and evaluate them to improve on one’s abilities. One consistency throughout the literature of educator training and interaction is the importance of self-reflection; Paterson and Chapman (2013), for example, argue that self-reflection that motivates an individual to learn from their experiences and is the key towards the maintenance and development of competency throughout their work practices. Others, such as or Hendrickx et al. (2016), mentions that reflective teachers who are aware of their influence on student behaviour can tailor their interactions to benefit their instructional practices.
According to Patil (2013), reflective practices are self-regulated processes that aim to enhance an individuals’ ability to communicate and make balanced decisions. Educational researchers, such as Valli (1997), describe reflective teachers as being individuals that can “look back on events, make judgments about them, and alter their teaching behaviors in light of craft, research, and ethical knowledge” (pg. 70). Other researchers argue that reflective action “involves intuition, emotion, and passion and is not something that can be neatly packaged as a set of techniques for teachers to use” (Zeichner & Liston 1996, pg. 9). These quotes would suggest that reflective practice in education is an ideal that pedagogics and educational researchers would encourage teachers to become accustomed to, but that the practical implementation of may be somewhat difficult to achieve.
Kay and Johnson (2002), speaking about the University of Washington’s teacher education programme, mention that the reflective seminars and completion of reflective portfolios are a useful method to provide support to student teachers in developing the skills necessary to reflect on their practices. Kay and Johnson (2002) do mention that the limitation of these methods is the way they categorise dimensions of reflection into a teachable concept, or that the use of typologies naturally constrain teachers towards ‘thinking like a teacher’. But, similar to Pratt and Collins (2010) view of the TPI, the concept of using this approach as a tool is quite useful. Without the opportunity and a way for teachers to systematically reflect on their instructional practices, they may be unable to view the importance of their instructional decisions, interactions, and relationships with students.
REFERENCES:
Bansal, S. (2016, May). TED Paris: How to fix a broken education system without any more money. Retrieved 1/7/2016 from TED.com at https://www.ted.com/talks/ seema_bansal_how_to_fix_a_broken_education_system_without_any_more_money?language=en.
Motoca, L. M., Farmer, T. W., Hamm, J. V., Byun, S. Y., Lee, D. L., Brooks, D. S., … & Moohr, M. M. (2014). Directed consultation, the SEALS model, and teachers’ classroom management. Journal of Emotional and Behavioural Disorders, 22(2): 119-129.
Bell, L. A. (1980). The School as an Organisation: a re‐appraisal. British Journal of Sociology of Education, 1(2), 183-192.
Hamzah, M., Yakop, F. M., Nordin, N. M., & Rahman, S. (2011). School as learning organisation: The role of principal’s transformational leadership in promoting teacher engagement. World Applied Sciences, 14, 58-63.
Mulford, B. (1998). Organisational learning and educational change. In A. Hargreaves, A. Lieberman, M. Fullan and D. Hopkins (Eds). International Handbook of Educational Change. Norwell, MA: Kluwer Academic Publishers.
Silins, H., Zarins, S., & Mulford, W. R. (2002). What characteristics and processes define a school as a learning organisation? Is this a useful concept to apply to schools? International Education Journal, 3(1): 24-32.
Johnston, C. (1998). Leadership and the learning organisation in self-managing schools. Unpublished doctoral dissertation, University of Melbourne, Victoria.
Brown, (2010). A mixed methods analysis of a mixed methods system: attitudes of Post Primary school Principals to internal/external evaluation: The Case of Ireland. Cited In McNamara, G., & O’Hara, J. (2012). From looking at our schools (LAOS) to whole school evaluation-management, leadership and learning (WSE-MLL): the evolution of inspection in Irish schools over the past decade. Educational Assessment, Evaluation and Accountability, 24(2), 79-97.
Collins, J. B., & Pratt, D. D. (2011). The teaching perspectives inventory at 10 years and 100,000 respondents: Reliability and validity of a teacher self-report inventory. Adult Education Quarterly, 61(4); 358-375.
Boud, D., Keogh, R., & Walker, D. (1985). Reflection, Turning Experience into Learning. Routledge.
Paterson, C., & Chapman, J. (2013). Enhancing skills of critical reflection to evidence learning in professional practice. Physical Therapy in Sport, 14(3): 133-138.
Hendrickx, M. M., Mainhard, M. T., Boor-Klip, H. J., Cillessen, A. H., & Brekelmans, M. (2016). Social dynamics in the classroom: Teacher support and conflict and the peer ecology. Teaching and Teacher Education, 53, 30-40.
Patil, S.S.J. (2013). Reflective practice in education. Global Online Electron Int Interdi Res J, 2(1): 356-358.
Valli, L. (1997). Listening to other voices: A description of teacher reflection in the United States. Peabody Journal of Education, 72(1): 67–88.
Zeichner, K. M., & &Liston, D. P. (1996). Reflective teaching: An introduction. Mahwah, New Jersey: Lawrence Erlbaum Associates.
Johnson, B.R., & Kay, A.J. (2002). Mixed Methods Research: A Research Paradigm whose Time Has Come. Educational Researcher, 33(7): 14-26.









You must be logged in to post a comment.