National Doctors Day is celebrated nationwide, every year, on the 1st of July. But why? This is to express our gratitude towards doctors and physicians for their service towards our well-being. Legendary physician and the second Chief Minister of West Bengal, Dr Bidhan Chandra Roy was born on the 1st of July in Patna, Bihar in 1882 and coincidentally died on the very same date in the year 1962. In 1961, Dr Roy was conferred with the nation’s highest civilian award, Bharat Ratna. Doctors day in India was established in 1991 in honour of his birth and death anniversary.
Well, Doctors day is celebrated every year on the 1st of July but this year another day was observed, by the doctors of IMA (Indian Medical Association) on 18th of June, NATIONAL PROTEST DAY. Doctors came together against the assaults on doctors in COVID wards. IMA observed nationwide protests demanding central law to protect doctors against violence.
Doctors and healthcare workers held placards and raised slogans like doctors bachao desh bachao (save doctors, save nation) and save the saviour. Doctors and medical staff at the IMA office in Hyderabad protested wearing black badges. Doctors from AIIMS Delhi and IMA unit, Ludhiana also took part in the agitations. Various state-level protests were taking place for a long time.
Why are these protests taking place?
Let me brief you here
Bhopal: A local politician was seen screaming at a Bhopal doctor who couldn’t save the life of a patient who was bought to the hospital at an oxygen level of 30. This left the doctor in tears and he was demoralised to the extent that he wanted to resign.
Guwahati: A doctor at a coronavirus facility in Assam was punched, kicked, and pounded with metal trash cans and bricks, by the relatives of a Covid patient who had died, allegedly due to oxygen shortage. Locals also assaulted the doctor who was then hospitalised.
Kerala: A police official allegedly attacked a doctor in the Alappuzha district. The official is accused of slapping Dr Rahul Mathew, who was working the night shift at the Mavelikkara district hospital, after the former’s mother, a COVID-19 patient, was brought dead to the hospitals. Doctors protest for the non-arrest.
And many more such cases went viral on social media. Assaults on doctors might not make it to the news daily, but take place every day.
What exactly did they do to get such treatment?
Grinded in high school, cracked NEET, spent 7-8 years working hard and studying in college, paid a hefty amount of fees to medical colleges or even took loans for their studies.
Who does that? Their fault, right?
Image source: Google | Image by: BusinessToday.In
During COVID lockdown when most of us were busy making dalgona coffee and baking cakes, they were out there in scorching heat, wearing PPE kits dealing with patients. Burning the candle at both ends, forgetting they have a life of their own, forgetting they have a family waiting for them, isolating themselves from their own family members, in their own houses to protect their families from contracting the virus, more than 500 doctors died during COVID, trying to save our lives. But why, just to save us. Imagine how demoralising it is for them to get beaten up by the ones they’re working for.
What is the probable reason?
Lack of infrastructure
Manpower
Laws in place
Security arrangements
Lack of infrastructure
The shortfall of ICUs, no beds for patients, dearth of oxygen support, the inadequacy of medicines, caretakers bound to wait in long queues for medicines at dispensaries, patients gasping outside hospitals, black marketing of almost everything required for a person to recover, our health infrastructure was crippling.
Image source: Google | Image by: The Times Of India
Manpower
Along with the tools used to help fight COVID, there is a paucity of our warriors too. There should be at least one doctor per 1000 patients according to WHO, whereas in India there is one doctor who attends more than 1445 patients. Not just doctors, the suggested number of nurses per 1000 patients is at least 3, there are just 1.7 in India (43% less than WHO standards). This leads to overworking of doctors and medical staff ignoring their basic requirements like sleep and a proper diet.
Laws in place
Medicare Service Persons and Medicare Service Institutions (Prevention of Violence and Damage to Property) Act, also known as the Medical protection act is there in at least 19 states, which when breached can lead to an imprisonment of up to 3 years and a fine of INR 50,000. Damage to any medical devices and equipment is a punishable offence and offenders are liable to pay twice the amount of the damaged equipment’s cost.
The Act, however, fails to really protect doctors because it features neither in the Indian Penal Code (IPC) nor in the Code of Criminal Procedure (CrPC). This makes it difficult for victims to approach the police for help or the latter to file a complaint against suspects.
Security arrangements
Doctors are not politicians with scores of gunmen and bouncers around them, who will assure their safety? Due to lack of security at hospitals and clinics, doctors and other staff are the soft targets for unhappy relatives and agitated patients.
Stepping into doctor’s shoes
Imagine yourself as a teacher who fears being beaten up to death by parents for their child’s poor performance at a test, will you even be willing to teach anymore with the same zest. I don’t think so. Hospitals are understaffed, doctors are overworked, patients are overwhelmed.
But this isn’t the fault of our doctors. They are going an extra mile in order to save as many patients as they can, making 3 patients share a bed or switching oxygen support among patients, they have our best interest at heart.
Doctors are not supposed to be accountable for the paralyzed infrastructure, that is where the leaders we vote for come into play. They’re made to work for 15+ hours at a stretch that too in a harsh environment, in a place they no longer feel safe or comfortable in.
What do doctors want?
All they want is for the government to sit with them and consider their problems.
For a law to protect their lives so that they can continue with their duties towards the nation. The implementation of existing laws.
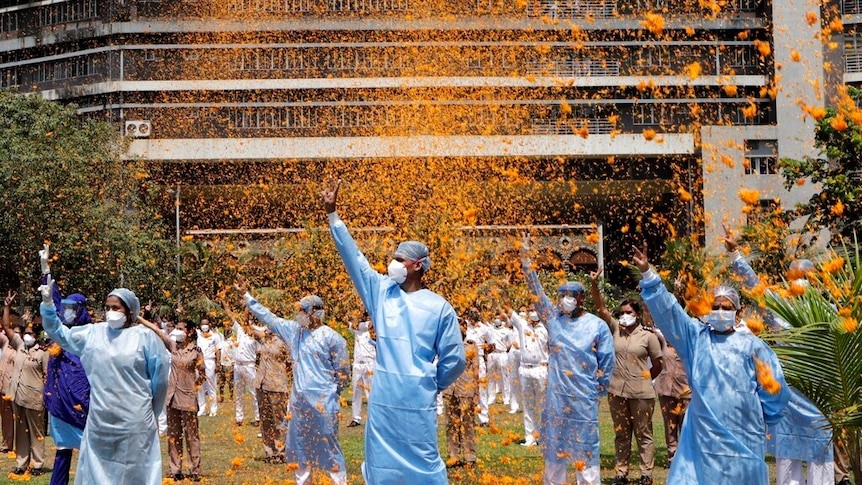
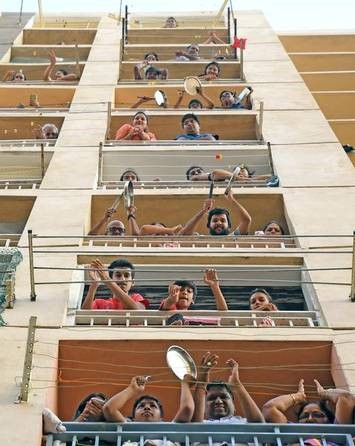
They don’t demand banging of thalis from our balconies or something like that in order to pay our respect, they didn’t ask for showering of flowers upon them for their service, all they’re asking for is to be able to practice in a safe environment where they’re worried for patients’ life, not scared of getting beaten up by sticks.
Image source: Google | Image by: Anjana Pasricha ( VoA)
We were always raised to believe doctors are God on land. Saving our life, giving us a new one at times, while risking their own. What they now want is not godly, but at least a humanly manner.
How can we help?
First and foremost, don’t be someone they need protection from. i.e. don’t be an assaulter.
Secondly, don’t ignore if you see someone being unfair toward them. Raise your voice, report if you see something like this.
A simple realisation that we can trust our doctors can do wonders.
Lastly, don’t forget they’re humans too. Thank them, pay your respect, or at least, just don’t be a jerk.
This Doctors day, I bet Dr Bidhan Chandra wouldn’t be proud of our country treating its doctors and medical staff like this.
Let’s all come together and promise that we’ll make the world a better place to live for our selfless human beings. We owe them.
Ending here with a salute to any doctor or an aspiring doctor reading this, and a sincere tribute to the warriors that lost their lives.
Doctor and a stethoscope are synonymous with each other. A stethoscope is doctor’s best buddy. Hung around one’s neck, it gives doctor his identity. It is basically an instrument used to listen sounds made by heart, lungs or intestines and blood flow in veins and arteries. Let’s read how a young doctor’s shyness led to its invention which proved to be path breaking in field of medical diagnosis.
Born in 1781, a young French doctor, Rene Laennec got inspired to become a doctor when his mother passed away due to tuberculosis. He was a learnt man who studied medicine under famous physicians Dupuytren and Joan Nicholas Corvisat.
Corvisat strongly believed in diagnosing a patient by listening to heart sounds. In those days (early 1800s), it was common for a doctor to listen one’s heart beat by pressing his head directly on patient’s chest or back.
In 1816, as a part of his training, Laennec was told to examine a young overweight woman who was having heart problem. Laennec felt shy as well as uncomfortable thinking about using the traditional method. At that moment, he thought of a way. He rolled a quire of paper into a cylinder and placed one end on the chest of the patient and other end to his ear. And much to his surprise, he perceived sounds better than the other traditional method.
Successful in his impromptu experiment, Laennec devised a wooden version. It was 25 cm by 2.5 cm and could be carried around. He named it STETHOSCOPE which was derieved from a greek word sthethos( meaning chest) and scopos (meaning examination). Gradually, its use spread across Europe and US. But unfortunately Laennec died in 1826 at the age of 45 due to the same disease, as of his mother, tuberculosis.
Till date, various refinements have been made to original one. The major changes were brought by a Harward Professor, David Littmann in 1960s. He made a lighter version with better acoustics.
Littmann stethoscope are no doubt, the gold standard and used worldwide by doctors. But Laennec’s invention proved to be major milestone in the history of medical sciences.
Many of us must be unaware about this but have a knowledge always pays of.
Biomedical Waste Management & Handling Rules, 1998 (“1998 Rules”) in India govern the handling, disposal and management of bio-medical waste (“BM Waste”)in India have been notified by the Central Government in the exercise of the powers conferred by Section 6,8 & 25 of the Environmental Protection Act, 1986. These rules provide for the framework of the management and Handling of disposal and scientific management of BM Waste
In wake of the COVID-19 pandemic, the Centre Pollution Control Board (“CPCB”) recently issued guidelines dated March 27, 2020 for handling, treatment and safe disposal of BM Waste generated during treatment, diagnosis and quarantine of patients confirmed or suspected to have COVID-19 (“Guidelines”).
The Guidelines have been necessitated due to the super infectious nature of the Novel corona virus and provide for a mechanism for the segregation, packaging, transportation, storage and disposal of BM Waste in order to avoid further spread of the virus through BM Waste.
So what do you mean by the BM Waste and what are the categories of BM Waste that the hospitals generate?
The Bio-Medical Waste Management Rules 2016[1] (“2016 Rules”) define the BM Waste as any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or research activities pertaining thereto or in the production or testing of biological or in health camps, including the categories mentioned in Schedule I the 2016 Rules.
The 2016 Rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form. The next imminent question that comes to our minds is what are the categories of BM Waste that the hospitals generate?
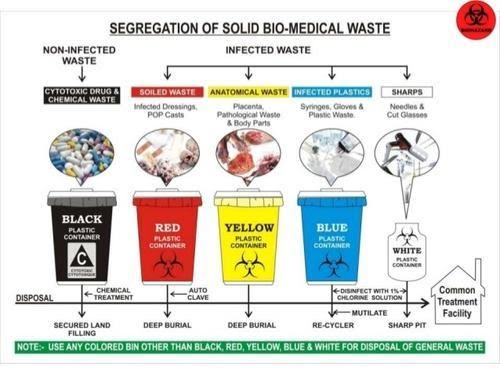
BM Waste generated from a hospital could be human anatomical waste, animal waste- microbiology & biotechnology, waste sharps, discarded medicines and cytotoxic drugs, solid & liquid waste.
Now that we know what’s the meaning and various categories of BM Waste, the most pertinent question arises that how is it supposed to be treated and disposed of by the hospitals in India during the ongoing COVID-19 pandemic?
While the hospitals in their usual course deal with the segregation, management and storage of BM Waste, the situation in times of COVID-19 is extraordinary the reason being the highly contagious nature of the virus and also it’s transmission cycle and multiplicity rate.
As the hospitals are being flooded with the suspected and confirmed cases, the Ministry of Health and family welfare (“MoHFW”) and the CPCB have issued various guidelines for the handling and management of waste generated from the COVID-19 facilities.
Under the 2016 Rules, while the hospitals are required to ensure that there is a secured location within its premises for a spill/pilferage free storage of segregated BM Waste in labelled/coloured bags or containers, the duty to transport the stored BM Waste from the hospital premises onwards to the common BM Waste treatment and disposal facility is of an ‘operator’ as defined in the Rules.
Specifically, in wake of COVID-19, the CPCB has issued Revision 1 to the Guidelines dated March 25, 2020 for Handling, Treatment and Disposal of Waste Generated during Treatment/Diagnosis/ Quarantine of COVID-19 Patients (“CPCB Guidelines”).
[2] The said CPCB Guidelines inter-alia, state that hospitals are required to depute separate BM Waste sanitation workers to COVID-19 isolation wards and maintain records of all waste generated in such isolation wards and ensure that the BWM generated is collected and separately stored in separate leakproof color-coded double layered bags or bins /containers labelled as “COVID-19 waste” as per the 1998 Rules and the Guidelines.
In fact the Bombay High Court in a recent pending public interest litigation has, while issuing notices to local municipal corporations and the State Pollution Control Board, also directed the Maharashtra government to clarify whether it was ensuring that all COVID-19 related biomedical waste generated in the state was being disposed of in a safe manner[3].
Now that we have a thorough understanding of how the BM Waste is supposed to be treated and disposed of the most important and the widely discussed about topic is that what are the measures that a hospital is required to take for the safety of its employees doctors, nurses and other support staff who are known as the (“healthcare personnel”) from the dangerous diseases like COVID-19?
In order to answer this pertinent question which is often there in the limelight, one must keep in mind that the Healthcare personnel who are the Frontline workers have a high risk of contracting the COVID-19.
While the hospitals are taking precautions and measures to control any spread of infection within the premises, it is particularly difficult given the highly super-infectious nature and hyper-speed feature of the virus. Due to this feature it spreads widely and it becomes a bit difficult to contain it in an over-crowded environment but it’s not impossible to achieve that as we all have been deterrent enough to contain it’s spread but still there is always scope for improvement.
The first steps towards controlling the spread of a virus is personal protective equipment also known as PPE which should preferably be a two-layered fluid-resistant apron and basic items like N-95 masks, face shield, full cover gowns and sanitisers but the same are rendered ineffective against the COVID-19 if the quality of these equipments is not up to the standard as required.
Greater emphasis is also to be laid upon the proper training and awareness of healthcare personnel towards proper use and disposal of the equipment. The spread of the COVID-19 virus is also particularly fast due to the heavy load of asymptomatic patients coming into the hospital and hence a greater need for the formulation of national COVID-19 protocol.
The MoHFW has vide its revised guidelines for clinical management of COVID-19 dated March 31, 2020[4] (“Clinical Management Guidelines”) impressed upon strict compliance of Infection prevention control (IPC) protocol for Hospitals and a consequent effect of the same is prevention and management of COVID-19 in the hospital staff.
This protocol inter-alia, standard precautions such as hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin, prevention of needle-stick or sharps injury, safe waste management, cleaning and disinfection of equipment and cleaning of the environment around a COVID-19 patient.
The 2016 Rules also provide as follows that in order to and for ensuring the safety of the healthcare workers and others involved in the segregation and pre-treatment of BM Waste, the hospital is required to train to all its healthcare workers, immunise them for protection against diseases which likely to be transmitted by handling of BM Waste, in the manner as prescribed in the National Immunisation Policy[5].
Also, hospitals are required to ensure occupational safety of all its health care workers and others involved in handling of BM Waste by providing appropriate and adequate PPE and also they must conduct health check ups at the time of induction and at least once in a year maintain the records for the same.
Now due to the pandemic if one is an employee ie the Healthcare personnel of the hospital one must understand the Legal aspect and angle also and the most important aspect of all is that what is the Legal obligations of the hospital, if and when an employee of the hospital tests positive for COVID-19.
Let’s answer this as it’s the most crucial and critical aspect. The present COVID-19 pandemic is an unprecedented event and is unlike any other infectious disease known to mankind and the medical world which is yet to fully decipher its modus operandi of infecting humans.
In a hypothetical situation wherein a hospital employee contracts COVID-19, it will be imperative for the employee in such a situation to establish that his possible exposure to COVID-19 was in the Hospital itself not in the community after considering that the employee is spending time outside as well apart from the hospital premises.
While in an ideal case, if it is proved that a hospital staff has contracted it ,i.e., it shall amount to ‘a hospital acquired infection’, then the hospital would be ordinarily liable. However, in the case of COVID-19 since it is seemingly impossible to trace down the exact source of the infection, in absence of such evidence and in light of utmost safety measures and precautions taken by the hospitals as per the guidelines, fastening of any liability on the hospital would be peculiarly difficult.
The defence available to the hospital may be culpability and negligence of the employee and proving that the hospital itself took all possible measures to avoid any mass spread of the infection.
The next relevant point to be analysed and answered is that when a Non COVID-19 patient contracts the virus during his term of being admitted in the hospital what are the Legal obligations of the hospital when this happens?
The National Consumer Dispute Redressal Commission in the matter of Apollo Emergency Hospital vs Dr. Bommakanti Sai Krishna & Anr.[6] observed that “As already observed, the infection occurred during the stay of the Complainant at the hospital. On the other hand, there is nothing to show that the source of infection lay outside the hospital. Thus, there is preponderance of possibilities of the infection having been acquired in the hospital itself. We therefore, do not accept the contention that it was necessary for the Complainant to produce expert evidence to prove negligence on the part of the concerned doctors in the hospital.”
The afore-stated judgement implies a presumption of liability on the hospital that in cases where the probability of acquiring the infection is much higher inside the hospital than from other sources. However, the same may not apply in COVID cases in light of the peculiar difficulty of tracing the source of acquiring the COVID-19 infection. Therefore, the presumption rendered by the aforesaid judgement will not be ipso facto applicable to cases of COVID patients.
As we have discussed the various pertinent relevant questions another one is that what are the legal obligations of the hospital, if and when a patient is misdiagnosed positive or negative for COVID-19 by the hospital due to a fault in the COVID-19 rapid testing kit (“testing kits”)?
The liability of a hospital in cases of misdiagnosis depends on the methodology of procuring of testing kits. A hospital may procure testing kit either from third party manufacturer or may manufacture them internally i.e. by itself or its subsidiary.
In cases where the misdiagnosis is on account of faulty testing kit procured externally, the hospital cannot be held directly liable as the liability may be shifted upon the manufacturer.
In cases where the misdiagnosis is on account of faulty testing kit is due to testing kits produced internally the hospital may be liable subject to it being proved that the misdiagnosed patient was indeed positive. However, factors such as the success rate of any testing kit not being 100% may have an interplay in determining the liability.
We have to be aware of what are the Legal liability of a hospital in a situation where the hospital discharges a mild/very mild/pre-symptomatic COVID patient to ramp up the capacity for serious COVID-19 patients.
A hospital will not be held liable for a systematic discharge of a mild/very mild/pre-symptomatic/moderate COVID-19 patient as the same is directed by the Central Government. On May 8, 2020, the MoHFW released its revised policy for the discharge of COVID-19 patients.[7] This revised policy provides that hospitals can discharge mild/very mild/pre-symptomatic in accordance with the protocols given therein.
In the earlier advisory[8], COVID-19 patients could be discharged only after chest radiograph clearance, viral clearance in respiratory samples, and if two of the patient’s specimens were negative within a period of 24 hours. The discharged patient would then have to home quarantine themselves in accordance with the revised policy.
So what is the protocol to be followed by a Hospital while disposing of the dead bodies of the COVID-19 patients?
The corpses are a source of infection for healthcare personnel/ other patients and cannot be disposed of by usual methods of disposal and therefore, the MHFW issued guidelines dated March 15, 2020 on dead body management in COVID-19.[9] The guidelines provide inter-alia, the protocol to be followed at the time of removal from the isolation room or area, put in bio-hazard bag and disinfection. Further, all surfaces of the isolation area (floors, bed, railings, side tables, IV stand etc.) should be wiped with 1% Sodium Hypochlorite solution and then it should allow a contact time of 30 minutes, and allow it to air dry as well.
While treating patients infected with the COVID-19 virus, what is the protocol for the treatment?
The All India Institute of Medical Sciences (AIIMS) has issued clinical protocol dated April 21, 2020 for treatment of Covid-19 patients and states such as Madhya Pradesh and Delhi have directed Hospitals and health centres dedicated to treating COVID-19 patients to follow the said clinical protocol.[10]
Treatment must be affordable for all. One must know whether or not there is a standardisation of costs of treatment of a COVID-19 for private hospitals?
Government hospitals are reaching their intake capacities and for that reason COVID-19 patients have been resorting to treatment in private hospitals. While some private hospitals are charging exorbitant amounts as costs of treatment, the same is worrying not just for the patients but also to the insurers.[11]
In a first, the State government of Maharashtra has capped treatment costs in private hospitals for people without medical insurance and for other patients, the capped prices will come into effect once they exhaust their medical insurance cover.[12]
The Hon’ble Gujarat High Court has vide its order dated May 22, 2020 directed the state government to issue a notification making it mandatory for all multi-speciality hospitals private/ corporate hospitals in Ahmedabad and on its outskirts to reserve 50% of their beds (or such other capacity as maybe specified by the state government) for COVID-19 patients.
In view of the same, the Government of Gujarat may come up with similar caps on costs as Maharashtra.[13] The Hon’ble Gujarat High Court also observed that the certain private hospitals authorised by the government to treat COVID-19 patients in Ahmedabad are charging exorbitant fees which is unaffordable for a massive section of the society and directed the state government to ensure that private hospitals do not charge exorbitant fees. [14]
Also in light of the same The Hon’ble Bombay High Court recently directed a charitable hospital to make court deposit of monies in a case pertaining to levy of exorbitant charges for treatment of COVID-19 patients belonging to poor strata of the society despite reserving 20% of its beds for poor and the needy.[15]











You must be logged in to post a comment.