The biggest question among the Corona virus epidemic is about the opening of schools and colleges. Some people are in favor of opening the school and many are against it. Meanwhile, a survey has revealed shocking results. The survey has been conducted by the Education Department of the state Haryana adjacent to Delhi.
In this survey of Haryana Education Department, it has been found that about 85% of the students of class 10th and 12th in the state are in favor of opening school from September 2020. Despite the dangers of the Corona epidemic, these parents are ready to send their children to school.
The survey was conducted online by the state school education department. In this, parents of a total of 76,019 students of class 10th and 12th of various government schools of the state attended. It included a few schools from all the 22 districts of the state.
What questions were asked from parents These four questions were asked by the education department to all parents –
Should schools be opened by September 2020?
Are parents ready to send their children to school from September 2020?
Have any of your family members conducted the Kovid test?
Have any of your family members been found to be Kovid positive? … so how will the schools be opened now.
An Education Department official said that ‘most of the students of 10th-12th students are in favor of opening of schools. Therefore, the department has decided to run trial run by opening two schools in different districts first. Government Senior Secondary School in Karnal and Government High School in Sonepat will be opened for four days. Dates will be revealed soon. ‘ In these four days, every movement of the school will be recorded on cameras. How students come to school, how they enter, how classes attend, or not touch each other, how they get out of school .. All these things will be recorded. Classes will be held in small groups instead of classrooms. After the trial, a team of seven members of the education department, including health and hygiene experts, will watch these video recordings to see if all the rules are being followed. If there is a shortage, teachers will be asked to remove it the very next day. These recordings will be shown to every teacher before school opens. The education department is preparing to open schools for class 10th and 12th from September 21.
Students have to submit written consent of their parents for this. An official of the Directorate of School Education has told that the ‘School Management Committee will conduct a survey from the parents of all the students from class 9th to 12th. If 60 percent or more of the parents are in favor of opening the school, it will be recorded in the school register. However, all these things are still in the planning stage.
A study published in a medical journal has revealed that SARS-CoV-2, which causes Covid-19, has undergone multiple mutations in its “spike proteins”. This is the protein that gives the virus the ability to infiltrate the human cells. Once this occurs, the virus starts replicating, which leads to infection.
The paper published in Journal of Laboratory Physicians was based on an analysis of 1,604 spike proteins extracted from 1,325 complete genomes and 279 partial spike coding sequences of SARS-CoV-2 available at National Center for Biotechnology Information (NCBI) in the US till May 1.
Dr Sarman Singh, the lead author of the study, said they found 12 mutations in the spike proteins, six of which were novel mutations. “One deletion was also found in an Indian strain (MT012098.1). Deletion means change in the genetic structure of the virus. We don’t know how it will affect the virulence of the disease though,” he added.
The maximum genetic mutations were observed in spike proteins extracted from genomes of SARS-CoV-2 from the US, the experts said. “Viruses are known to mutate or change their genetic structure upon exposure to different environments. But in this case, the change is happening quite fast. We are not sure how it will affect the disease spread,” Singh said.
The others participants of the study included experts from Infectious Diseases and Immunity in Global Health Programme, Research Institute of McGill University Health Center, and McGill International TB Center, Canada. The study said spike protein was the major target for vaccine development, but several mutations were predicted in the antigenic epitopes across all genomes available globally.
“The emergence of various mutations within a short period might result in conformational changes in the protein structure, which suggests that developing a universal vaccine could be a challenging task,” the study added. Mutation was also found in the antigens responsible for producing antibodies, indicating that the patients infected with the mutants would have very low or nil antibodies.
Recently, Hong Kong reported a case of re-infection due to Covid-19. Similar cases have also been documented in the US and India. “Even if a person gets Covid-19 again due to a mutated strain of the virus, the likelihood of severe symptoms would be less as seen in the patient in Hong Kong. This is because the antibodies against one strain of Covid-19 can offer protection against the mutated virus too. However, further scientific study and analysis is needed to ascertain this. The disease is new and we are still learning about it,” said a virologist from Maulana Azad Medical College.
In Delhi, the cases of Covid-19 had dipped significantly in July. However, it has started rising over the past few days. While lack of social discipline and opening of the economy are two key factors, many doctors said a mutation of the virus could also be behind it. “Multiple strains of the virus have been identified in the country, including the original one from Wuhan, China and the ones spreading in Europe,” said a doctor. The World Health Organization does not expect widespread vaccinations against COVID-19 until the middle of next year, said a spokeswomen, stressing the importance of rigorous checks on their effectiveness and safety.
The World Health Organization insisted Friday it would never endorse a vaccine that has not proven safe and effective, amid concerns over the rush to develop a jab for Covid-19. Across the globe, governments are hoping to deploy a vaccine as soon as possible against the virus, which has infected well over 26 million people, killed hundreds of thousands, upended millions of lives and wreaked havoc on the global economy.
Under normal procedures, test administrators must wait for months or years to verify that vaccine candidates are safe and efficacious. But as the pandemic continues to take a devastating toll, there has been massive pressure to roll out a vaccine quickly, sparking concerns that testing standards could be lowered. WHO chief Tedros Adhanom Ghebreyesus insisted that was not the case.
“WHO will not endorse a vaccine that is not effective and safe,” he told a virtual briefing.
He also took issue with the so-called anti-vax movement that has been stoking fears about the vaccines in development. They might be able to “build narratives to fight against vaccines, but the track record of vaccines tells its own story,” he said.
There are currently more than 30 candidate vaccines being tested on humans, with at least eight in final-stage Phase III trials, which typically involve tens of thousands of people. Unprecedented speed’ – “It is a very optimistic scenario because there’s a huge field of candidates,” WHO’s chief scientist Soumya Swaminathan told Friday’s briefing, emphasising that only around 10 percent of candidate vaccines succeed.
She explained that the “unprecedented speed of development of Covid vaccines” was largely enabled by prior investments in vaccine platforms for other diseases, which had been repurposed for use against the novel coronavirus. But she stressed, developers must not skip over the various phases of stringent testing.
“No vaccine is going to be mass-deployed before the regulators are confident and the governments are confident and that WHO is confident that these vaccines have met the minimum standards of safety and efficacy.” Tedros voiced hope that one would soon become available “so that the world can get back to norma.” But while the WHO has said it expects to see results from a range of Phase III trials by the end of the year, it on Friday tempered hopes that a vaccine is imminent.
Pointing to the massive challenge of manufacturing and rolling out vaccines to the billions around the world who need them, widespread vaccination is not expected to begin until the middle of 2021. Moral and economic imperative’ – Tedros stressed that, initially at least, supply would be limited.
“Priority must be given to vaccinating essential workers and those most at risk,” he said, stressing that “the first priority must be to vaccinate some people in all countries, rather than all people in some countries.” The WHO has set up a mechanism, known as Covax, aimed at ensuring a more equitable distribution of any future vaccines, but has struggled so far to raise the funds needed to provide for the 92 poor countries that have signed up. But Tedros hailed Friday that 78 high- and upper-middle income countries and economies have now confirmed they will participate, including Germany, Japan, Norway and the European Commission in just the past week. He pointed out that in an interconnected world, “the virus will continue to kill and the economic recovery globally will be delayed” if poorer countries are unable to gain access to a vaccine. Sharing equitably, he said, is “not just a moral imperative and a public health imperative, it’s also an economic imperative.”
Government of India is taking several steps to ensure that we are well prepared to face the challenges and threats posed by COVID-19. With active support of citizens of India, we have been able to mitigate the spread of the virus so far. One of the most important factors in the fight with the virus is to empower the citizens with accurate information and enable them to take precautions as per the advisories being issued by different Ministries. The COVID-19 Inter-Ministerial Notifications website serves this purpose efficiently by providing COVID-19 related notifications from various Ministries in a format that is accessible, built using the S3WaaS framework, that is secure & scalable.
India has faced the COVID-19 situation with fortitude and a spirit of self-reliance, that is evident in the fact that from zero production of Personal Protection Equipment (PPE) before March 2020, India today has created a capacity of producing 2 lakh PPE kits daily, which is also growing steadily. Additionally, India has demonstrated how it rises up to challenges and uncovers opportunities therein, as manifested in the re-purposing of various automobile sector industries to collaborate in the making of life-saving ventilators. The clarion call given by the Hon’ble PM to use these trying times to become Atmanirbhar (self-reliant) has been very well received to enable the resurgence of the Indian economy.
Unlock 1 Guidelines have been issued to enable resumption of economic activities while maintaining abundant caution thus allowing graded easing of restrictions. The Five pillars of Atmanirbhar Bharat focus on: • Economy • Infrastructure • System • Vibrant Demography and • Demand
The Five phases of Atmanirbhar Bharat are: • Phase-I: Businesses including MSMEs • Phase-II: Poor, including migrants and farmers • Phase-III: Agriculture • Phase-IV: New Horizons of Growth • Phase-V: Government Reforms and Enablers
The exemplary role played by India in the global fight against COVID-19 has been recognized and appreciated widely. The Union Minister of Health & Family Welfare Dr. Harsh Vardhan has been elected as Chair of the Executive Board of World Health Organization for the year 2020-21. This took place during the 147th session of the Executive Board, in a meeting that was held virtually. He takes over from Dr Hiroki Nakatani of Japan.
Atmanirbhar focuses on small scale and medium scale industries. It also focuses on the service sector. Development of business that has faced a downfall due to Covid-19 pandemic and bringing up of the nation is the primary aim of this scheme. It also involves development of the economy as a whole. Assisting farmers in providing some support to agriculture is also under this scheme.
These 5 phases are to be carried on With due attention has it involves the development of the economy. Assisting the migrants in reaching their destinations. They lacked income during this pandemic. Financial assistance also is to be provided to the migrants. Development of the infrastructure facilities in a better way.
Due to the pandemic, India suffered a greater loss in its income. this has been affected as the citizens lacked work reducing their income. It has affected the economy of the nation. Bringing back the economy is the main aim of this scheme. Nation can be developed through the propose implementation of this scheme.
Coronaviruses are a group of related RNA viruses that cause diseases in mammals and birds. In humans and birds, they cause respiratory tract infections that can range from mild to lethal. Mild illnesses in humans include some cases of the common cold (which is also caused by other viruses, predominantly rhinoviruses), while more lethal varieties can cause SARS, MERS, and COVID-19. In cows and pigs they cause diarrhea, while in mice they cause hepatitis and encephalomyelitis. There are as yet no vaccines or antiviral drugs to prevent or treat human coronavirus infections.Coronaviruses are a group of related RNA viruses that cause diseases in mammals and birds. In humans and birds, they cause respiratory tract infections that can range from mild to lethal. Mild illnesses in humans include some cases of the common cold (which is also caused by other viruses, predominantly rhinoviruses), while more lethal varieties can cause SARS, MERS, and COVID-19. In cows and pigs they cause diarrhea, while in mice they cause hepatitis and encephalomyelitis. There are as yet no vaccines or antiviral drugs to prevent or treat human coronavirus infections.
Etymology:- The name “coronavirus” is derived from Latin corona, meaning “crown” or “wreath”, itself a borrowing from Greek κορώνη korṓnē, “garland, wreath”.The name was coined by June Almeida and David Tyrrell who first observed and studied human coronaviruses.The word was first used in print in 1968 by an informal group of virologists in the journal Nature to designate the new family of viruses.The name refers to the characteristic appearance of virions (the infective form of the virus) by electron microscopy, which have a fringe of large, bulbous surface projections creating an image reminiscent of the solar corona or halo.This morphology is created by the viral spike peplomers, which are proteins on the surface of the virus.
The earliest reports of an illness caused by a coronavirus occurred in the late 1920s, when an acute respiratory infection of domesticated chickens emerged in North America.Arthur Schalk and M.C. Hawn in 1931 made the first detailed report which described a new respiratory infection of chickens in North Dakota. The infection of new-born chicks was characterized by gasping and listlessness with high mortality rates of 40–90%.Leland David Bushnell and Carl Alfred Brandly isolated the virus in 1933.The virus was then known as infectious bronchitis virus (IBV). Charles D. Hudson and Fred Robert Beaudette cultivated the virus for the first time in 1937.The specimen came to be known as the Beaudette strain. In the late 1940s, two more animal coronaviruses, JHM that causes brain disease (murine encephalitis) and mouse hepatitis virus (MHV) that causes hepatitis in mice were discovered. It was not realized at the time that these three different viruses were related.
Human coronaviruses were discovered in the 1960susing two different methods in the United Kingdom and the United States.E.C. Kendall, Malcolm Bynoe, and David Tyrrell working at the Common Cold Unit of the British Medical Research Council collected a unique common cold virus designated B814 in 1961.The virus could not be cultivated using standard techniques which had successfully cultivated rhinoviruses, adenoviruses and other known common cold viruses. In 1965, Tyrrell and Bynoe successfully cultivated the novel virus by serially passing it through organ culture of human embryonic trachea.The new cultivating method was introduced to the lab by Bertil Hoorn.The isolated virus when intranasally inoculated into volunteers caused a cold and was inactivated by ether which indicated it had a lipid envelope.Dorothy Hamre and John Procknow at the University of Chicago isolated a novel cold from medical students in 1962. They isolated and grew the virus in kidney tissue culture, assigning it as 229E. The novel virus caused a cold in volunteers and was inactivated by ether similarly as B814.Scottish virologist June Almeida at St. Thomas Hospital in London, collaborating with Tyrrell, compared the structures of IBV, B814 and 229E in 1967.
Using electron microscopy the three viruses were shown to be morphologically related by their general shape and distinctive club-like spikes.A research group at the National Institute of Health the same year was able to isolate another member of this new group of viruses using organ culture and named one of the samples OC43 (OC for organ culture) Like B814, 229E, and IBV, the novel cold virus OC43 had distinctive club-like spikes when observed with the electron microscope. The IBV-like novel cold viruses were soon shown to be also morphologically related to the mouse hepatitis virus.This new group of viruses were named coronaviruses after their distinctive morphological appearance.Human coronavirus 229E and human coronavirus OC43 continued to be studied in subsequent decade.The coronavirus strain B814 was lost. It is not known which present human coronavirus it was.Other human coronaviruses have since been identified, including SARS-CoV in 2003, HCoV NL63 in 2003, HCoV HKU1 in 2004, MERS-CoV in 2013, and SARS-CoV-2 in 2020.There have also been a large number of animal coronaviruses identified since the 1960s.
Microbiology :- Coronaviruses are large, roughly spherical particles with bulbous surface projections.The average diameter of the virus particles is around 125 nm (.125 μm). The diameter of the envelope is 85 nm and the spikes are 20 nm long. The envelope of the virus in electron micrographs appears as a distinct pair of electron-dense shells (shells that are relatively opaque to the electron beam used to scan the virus particle). The viral envelope consists of a lipid bilayer, in which the membrane (M), envelope (E) and spike (S) structural proteins are anchored.[47] The ratio of E:S:M in the lipid bilayer is approximately 1:20:300.On average a coronavirus particle has 74 surface spikes.A subset of coronaviruses (specifically the members of betacoronavirus subgroup A) also have a shorter spike-like surface protein called hemagglutinin esterase (HE).
The coronavirus surface spikes are homotrimers of the S protein, which is composed of an S1 and S2 subunit. The homotrimeric S protein is a class I fusion protein which mediates the receptor binding and membrane fusion between the virus and host cell. The S1 subunit forms the head of the spike and has the receptor binding domain (RBD). The S2 subunit forms the stem which anchors the spike in the viral envelope and on protease activation enables fusion. The E and M protein are important in forming the viral envelope and maintaining its structural shape.
Inside the envelope, there is the nucleocapsid, which is formed from multiple copies of the nucleocapsid (N) protein, which are bound to the positive-sense single-stranded RNA genome in a continuous beads-on-a-string type conformation.The lipid bilayer envelope, membrane proteins, and nucleocapsid protect the virus when it is outside the host cell.
Genome See also: Severe acute respiratory syndrome-related coronavirus § Genome
Schematic representation of the genome organization and functional domains of S protein for SARS-CoV and MERS-CoV Coronaviruses contain a positive-sense, single-stranded RNA genome. The genome size for coronaviruses ranges from 26.4 to 31.7 kilobases.[9] The genome size is one of the largest among RNA viruses. The genome has a 5′ methylated cap and a 3′ polyadenylated tail.
The genome organization for a coronavirus is 5′-leader-UTR-replicase (ORF1ab)-spike (S)-envelope (E)-membrane (M)-nucleocapsid (N)-3′UTR-poly (A) tail. The open reading frames 1a and 1b, which occupy the first two-thirds of the genome, encode the replicase polyprotein (pp1ab). The replicase polyprotein self cleaves to form 16 nonstructural proteins (nsp1–nsp16).
The later reading frames encode the four major structural proteins: spike, envelope, membrane, and nucleocapsid. Interspersed between these reading frames are the reading frames for the accessory proteins. The number of accessory proteins and their function is unique depending on the specific coronavirus.
Replication cycle Cell entry
The life cycle of a coronavirus Infection begins when the viral spike protein attaches to its complementary host cell receptor. After attachment, a protease of the host cell cleaves and activates the receptor-attached spike protein. Depending on the host cell protease available, cleavage and activation allows the virus to enter the host cell by endocytosis or direct fusion of the viral envelop with the host membrane. Genome translation On entry into the host cell, the virus particle is uncoated, and its genome enters the cell cytoplasm. The coronavirus RNA genome has a 5′ methylated cap and a 3′ polyadenylated tail, which allows it to act like a messenger RNA and be directly translated by the host cell’s ribosomes. The host ribosomes translate the initial overlapping open reading frames ORF1a and ORF1b of the virus genome into two large overlapping polyproteins, pp1a and pp1ab. SARS-CoV genome and proteins The larger polyprotein pp1ab is a result of a -1 ribosomal frameshift caused by a slippery sequence (UUUAAAC) and a downstream RNA pseudoknot at the end of open reading frame ORF1a.The ribosomal frameshift allows for the continuous translation of ORF1a followed by ORF1b.
The polyproteins have their own proteases, PLpro (nsp3) and 3CLpro (nsp5), which cleave the polyproteins at different specific sites. The cleavage of polyprotein pp1ab yields 16 nonstructural proteins (nsp1 to nsp16). Product proteins include various replication proteins such as RNA-dependent RNA polymerase (nsp12), RNA helicase (nsp13), and exoribonuclease (nsp14).
Replicase-transcriptase
Replicase-transcriptase complex A number of the nonstructural proteins coalesce to form a multi-protein replicase-transcriptase complex. The main replicase-transcriptase protein is the RNA-dependent RNA polymerase (RdRp). It is directly involved in the replication and transcription of RNA from an RNA strand. The other nonstructural proteins in the complex assist in the replication and transcription process. The exoribonuclease nonstructural protein, for instance, provides extra fidelity to replication by providing a proofreading function which the RNA-dependent RNA polymerase lacks.
Replication – One of the main functions of the complex is to replicate the viral genome. RdRp directly mediates the synthesis of negative-sense genomic RNA from the positive-sense genomic RNA. This is followed by the replication of positive-sense genomic RNA from the negative-sense genomic RNA.
Transcription of nested mRNAs
Nested set of subgenomic mRNAs Transcription – The other important function of the complex is to transcribe the viral genome. RdRp directly mediates the synthesis of negative-sense subgenomic RNA molecules from the positive-sense genomic RNA. This process is followed by the transcription of these negative-sense subgenomic RNA molecules to their corresponding positive-sense mRNAs.The subgenomic mRNAs form a “nested set” which have a common 5′-head and partially duplicate 3′-end. Recombination – The replicase-transcriptase complex is also capable of genetic recombination when at least two viral genomes are present in the same infected cell.RNA recombination appears to be a major driving force in determining genetic variability within a coronavirus species, the capability of a coronavirus species to jump from one host to another and, infrequently, in determining the emergence of novel coronaviruses.The exact mechanism of recombination in coronaviruses is unclear, but likely involves template switching during genome replication. Assembly and release The replicated positive-sense genomic RNA becomes the genome of the progeny viruses. The mRNAs are gene transcripts of the last third of the virus genome after the initial overlapping reading frame. These mRNAs are translated by the host’s ribosomes into the structural proteins and a number of accessory proteins.RNA translation occurs inside the endoplasmic reticulum. The viral structural proteins S, E, and M move along the secretory pathway into the Golgi intermediate compartment. There, the M proteins direct most protein-protein interactions required for assembly of viruses following its binding to the nucleocapsid. Progeny viruses are then released from the host cell by exocytosis through secretory vesicles. Once released the viruses can infect other host cells. Transmission Infected carriers are able to shed viruses into the environment. The interaction of the coronavirus spike protein with its complementary cell receptor is central in determining the tissue tropism, infectivity, and species range of the released virus.Coronaviruses mainly target epithelial cells.They are transmitted from one host to another host, depending on the coronavirus species, by either an aerosol, fomite, or fecal-oral route. Human coronaviruses infect the epithelial cells of the respiratory tract, while animal coronaviruses generally infect the epithelial cells of the digestive tract.SARS coronavirus, for example, infects via an aerosol route,the human epithelial cells of the lungs by binding to the angiotensin-converting enzyme 2 (ACE2) receptor.Transmissible gastroenteritis coronavirus (TGEV) infects, via a fecal-oral route,the pig epithelial cells of the digestive tract by binding to the alanine aminopeptidase (APN) receptor.
Classification :- The scientific name for coronavirus is Orthocoronavirinae or Coronavirinae.
Coronaviruses belong to the family of Coronaviridae, order Nidovirales, and realm Riboviria.They are divided into alphacoronaviruses and betacoronaviruses which infect mammals – and gammacoronaviruses and deltacoronaviruses, which primarily infect birds.
Genus: Alphacoronavirus;type species: Alphacoronavirus 1 (TGEV) Species: Alphacoronavirus 1, Human coronavirus 229E, Human coronavirus NL63, Miniopterus bat coronavirus 1, Miniopterus bat coronavirus HKU8, Porcine epidemic diarrhea virus, Rhinolophus bat coronavirus HKU2, Scotophilus bat coronavirus 512 Genus Betacoronavirus;type species: Murine coronavirus (MHV) Species: Betacoronavirus 1 (Bovine Coronavirus, Human coronavirus OC43), Hedgehog coronavirus 1, Human coronavirus HKU1, Middle East respiratory syndrome-related coronavirus, Murine coronavirus, Pipistrellus bat coronavirus HKU5, Rousettus bat coronavirus HKU9, Severe acute respiratory syndrome-related coronavirus (SARS-CoV, SARS-CoV-2), Tylonycteris bat coronavirus HKU4 Genus Gammacoronavirus;type species: Avian coronavirus (IBV) Species: Avian coronavirus, Beluga whale coronavirus SW1 Genus Deltacoronavirus; type species: Bulbul coronavirus HKU11 Species: Bulbul coronavirus HKU11, Porcine coronavirus HKU15.
Origin :- The most recent common ancestor (MRCA) of all coronaviruses is estimated to have existed as recently as 8000 BCE, although some models place the common ancestor as far back as 55 million years or more, implying long term coevolution with bat and avian species.The most recent common ancestor of the alphacoronavirus line has been placed at about 2400 BCE, of the betacoronavirus line at 3300 BCE, of the gammacoronavirus line at 2800 BCE, and of the deltacoronavirus line at about 3000 BCE. Bats and birds, as warm-blooded flying vertebrates, are an ideal natural reservoir for the coronavirus gene pool (with bats the reservoir for alphacoronaviruses and betacoronavirus – and birds the reservoir for gammacoronaviruses and deltacoronaviruses). The large number and global range of bat and avian species that host viruses has enabled extensive evolution and dissemination of coronaviruses.
Many human coronaviruses have their origin in bats.The human coronavirus NL63 shared a common ancestor with a bat coronavirus (ARCoV.2) between 1190 and 1449 CE.The human coronavirus 229E shared a common ancestor with a bat coronavirus (GhanaGrp1 Bt CoV) between 1686 and 1800 CE.More recently, alpaca coronavirus and human coronavirus 229E diverged sometime before 1960.MERS-CoV emerged in humans from bats through the intermediate host of camels.MERS-CoV, although related to several bat coronavirus species, appears to have diverged from these several centuries ago.The most closely related bat coronavirus and SARS-CoV diverged in 1986.A possible path of evolution of SARS coronavirus and keen bat coronaviruses is that SARS-related coronaviruses coevolved in bats for a long time. The ancestors of SARS-CoV first infected leaf-nose bats of the genus Hipposideridae; subsequently, they spread to horseshoe bats in the species Rhinolophidae, then to Asian palm civets, and finally to humans. Unlike other betacoronaviruses, bovine coronavirus of the species Betacoronavirus 1 and subgenus Embecovirus is thought to have originated in rodents and not in bats. In the 1790s, equine coronavirus diverged from the bovine coronavirus after a cross-species jump.Later in the 1890s, human coronavirus OC43 diverged from bovine coronavirus after another cross-species spillover event.It is speculated that the flu pandemic of 1890 may have been caused by this spillover event, and not by the influenza virus, because of the related timing, neurological symptoms, and unknown causative agent of the pandemic.Besides causing respiratory infections, human coronavirus OC43 is also suspected of playing a role in neurological diseases.In the 1950s, the human coronavirus OC43 began to diverge into its present genotypes.Phylogentically, mouse hepatitis virus (Murine coronavirus), which infects the mouse’s liver and central nervous system is related to human coronavirus OC43 and bovine coronavirus. Human coronavirus HKU1, like the aforementioned viruses, also has its origins in rodents.
Prevention and treatment:- There are no vaccines or antiviral drugs to prevent or treat human coronavirus infections. Treatment is only supportive. A number of antiviral targets have been identified such as viral proteases, polymerases, and entry proteins. Drugs are in development which target these proteins and the different steps of viral replication. A number of vaccines using different methods are also under development for different human coronaviruses.
There are no antiviral drugs to treat animal coronaviruses.[citation needed] Vaccines are available for IBV, TGEV, and Canine CoV, although their effectiveness is limited. In the case of outbreaks of highly contagious animal coronaviruses, such as PEDV, measures such as destruction of entire herds of pigs may be used to prevent transmission to other herds.
Asia Cup 2020 officially postponed, ACC hopeful of hosting it in June 2021.The Asian Cricket Council on Thursday announced that the 2020 Asia Cup has been postponed. ACC stated that it is hopeful to conduct and schedule tournament on June 2021.
In the press release, ACC stated that the travel restrictions, different quarantine rules of countries, health risks and social distancing norms have posed as challenges to the conduct of the Asia Cup.The Asian Cricket Council on Thursday announced that the 2020 Asia Cup has been postponed. ACC stated that it will try to secure the window of June 2021 to schedule the tournament.
Right from the beginning the board was to organise the tournament as per the original schedule.However, travel restrictions, country-specific quarantine requirements, fundamental health risks and social distancing norms have posed as substantial challenges to the holding of the Asia Cup. Above all, the risks related to health and safety of participating players, support staff, commercial partners, fans and the cricketing community were deemed to be significant,” ACC quoted in the release.
The ACC is hopeful to schedule the Asia Cup in 2021 are looking for the June window to host the tournament.
” The Board, after careful consideration of all the above factors, has confirmed that the Asia Cup 2020 be postponed. Conducting the event with all due safety is major responsibility of ACC and the Board is hopeful that the tournament will be held in 2021. The ACC is currently working towards securing June 2021 as a option for the same,” quoted ACC.
ACC also cleared the air on the hosting nation of the next Asia Cup as it said the Pakistan Cricket Board has exchanged hosting rights with Sri Lanka Cricket Board.
“It can be possible that Sri Lanka hosts for the Asia Cup 2020, Pakistan Cricket Board (PCB), has exchanged hosting rights for the tournament with Sri Lanka Cricket (SLC). Through this arrangement, the SLC will now host the rescheduled Asia Cup expected in June 2021 while the PCB will host the Asia Cup 2022,” the ACC press release stated.
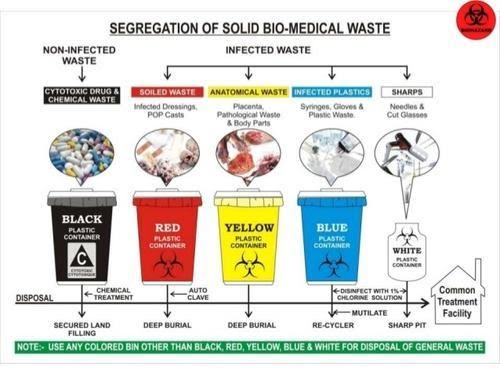
Biomedical Waste Management & Handling Rules, 1998 (“1998 Rules”) in India govern the handling, disposal and management of bio-medical waste (“BM Waste”)in India have been notified by the Central Government in the exercise of the powers conferred by Section 6,8 & 25 of the Environmental Protection Act, 1986. These rules provide for the framework of the management and Handling of disposal and scientific management of BM Waste
In wake of the COVID-19 pandemic, the Centre Pollution Control Board (“CPCB”) recently issued guidelines dated March 27, 2020 for handling, treatment and safe disposal of BM Waste generated during treatment, diagnosis and quarantine of patients confirmed or suspected to have COVID-19 (“Guidelines”).
The Guidelines have been necessitated due to the super infectious nature of the Novel corona virus and provide for a mechanism for the segregation, packaging, transportation, storage and disposal of BM Waste in order to avoid further spread of the virus through BM Waste.
So what do you mean by the BM Waste and what are the categories of BM Waste that the hospitals generate?
The Bio-Medical Waste Management Rules 2016[1] (“2016 Rules”) define the BM Waste as any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or research activities pertaining thereto or in the production or testing of biological or in health camps, including the categories mentioned in Schedule I the 2016 Rules.
The 2016 Rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form. The next imminent question that comes to our minds is what are the categories of BM Waste that the hospitals generate?
BM Waste generated from a hospital could be human anatomical waste, animal waste- microbiology & biotechnology, waste sharps, discarded medicines and cytotoxic drugs, solid & liquid waste.
Now that we know what’s the meaning and various categories of BM Waste, the most pertinent question arises that how is it supposed to be treated and disposed of by the hospitals in India during the ongoing COVID-19 pandemic?
While the hospitals in their usual course deal with the segregation, management and storage of BM Waste, the situation in times of COVID-19 is extraordinary the reason being the highly contagious nature of the virus and also it’s transmission cycle and multiplicity rate.
As the hospitals are being flooded with the suspected and confirmed cases, the Ministry of Health and family welfare (“MoHFW”) and the CPCB have issued various guidelines for the handling and management of waste generated from the COVID-19 facilities.
Under the 2016 Rules, while the hospitals are required to ensure that there is a secured location within its premises for a spill/pilferage free storage of segregated BM Waste in labelled/coloured bags or containers, the duty to transport the stored BM Waste from the hospital premises onwards to the common BM Waste treatment and disposal facility is of an ‘operator’ as defined in the Rules.
Specifically, in wake of COVID-19, the CPCB has issued Revision 1 to the Guidelines dated March 25, 2020 for Handling, Treatment and Disposal of Waste Generated during Treatment/Diagnosis/ Quarantine of COVID-19 Patients (“CPCB Guidelines”).
[2] The said CPCB Guidelines inter-alia, state that hospitals are required to depute separate BM Waste sanitation workers to COVID-19 isolation wards and maintain records of all waste generated in such isolation wards and ensure that the BWM generated is collected and separately stored in separate leakproof color-coded double layered bags or bins /containers labelled as “COVID-19 waste” as per the 1998 Rules and the Guidelines.
In fact the Bombay High Court in a recent pending public interest litigation has, while issuing notices to local municipal corporations and the State Pollution Control Board, also directed the Maharashtra government to clarify whether it was ensuring that all COVID-19 related biomedical waste generated in the state was being disposed of in a safe manner[3].
Now that we have a thorough understanding of how the BM Waste is supposed to be treated and disposed of the most important and the widely discussed about topic is that what are the measures that a hospital is required to take for the safety of its employees doctors, nurses and other support staff who are known as the (“healthcare personnel”) from the dangerous diseases like COVID-19?
In order to answer this pertinent question which is often there in the limelight, one must keep in mind that the Healthcare personnel who are the Frontline workers have a high risk of contracting the COVID-19.
While the hospitals are taking precautions and measures to control any spread of infection within the premises, it is particularly difficult given the highly super-infectious nature and hyper-speed feature of the virus. Due to this feature it spreads widely and it becomes a bit difficult to contain it in an over-crowded environment but it’s not impossible to achieve that as we all have been deterrent enough to contain it’s spread but still there is always scope for improvement.
The first steps towards controlling the spread of a virus is personal protective equipment also known as PPE which should preferably be a two-layered fluid-resistant apron and basic items like N-95 masks, face shield, full cover gowns and sanitisers but the same are rendered ineffective against the COVID-19 if the quality of these equipments is not up to the standard as required.
Greater emphasis is also to be laid upon the proper training and awareness of healthcare personnel towards proper use and disposal of the equipment. The spread of the COVID-19 virus is also particularly fast due to the heavy load of asymptomatic patients coming into the hospital and hence a greater need for the formulation of national COVID-19 protocol.
The MoHFW has vide its revised guidelines for clinical management of COVID-19 dated March 31, 2020[4] (“Clinical Management Guidelines”) impressed upon strict compliance of Infection prevention control (IPC) protocol for Hospitals and a consequent effect of the same is prevention and management of COVID-19 in the hospital staff.
This protocol inter-alia, standard precautions such as hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin, prevention of needle-stick or sharps injury, safe waste management, cleaning and disinfection of equipment and cleaning of the environment around a COVID-19 patient.
The 2016 Rules also provide as follows that in order to and for ensuring the safety of the healthcare workers and others involved in the segregation and pre-treatment of BM Waste, the hospital is required to train to all its healthcare workers, immunise them for protection against diseases which likely to be transmitted by handling of BM Waste, in the manner as prescribed in the National Immunisation Policy[5].
Also, hospitals are required to ensure occupational safety of all its health care workers and others involved in handling of BM Waste by providing appropriate and adequate PPE and also they must conduct health check ups at the time of induction and at least once in a year maintain the records for the same.
Now due to the pandemic if one is an employee ie the Healthcare personnel of the hospital one must understand the Legal aspect and angle also and the most important aspect of all is that what is the Legal obligations of the hospital, if and when an employee of the hospital tests positive for COVID-19.
Let’s answer this as it’s the most crucial and critical aspect. The present COVID-19 pandemic is an unprecedented event and is unlike any other infectious disease known to mankind and the medical world which is yet to fully decipher its modus operandi of infecting humans.
In a hypothetical situation wherein a hospital employee contracts COVID-19, it will be imperative for the employee in such a situation to establish that his possible exposure to COVID-19 was in the Hospital itself not in the community after considering that the employee is spending time outside as well apart from the hospital premises.
While in an ideal case, if it is proved that a hospital staff has contracted it ,i.e., it shall amount to ‘a hospital acquired infection’, then the hospital would be ordinarily liable. However, in the case of COVID-19 since it is seemingly impossible to trace down the exact source of the infection, in absence of such evidence and in light of utmost safety measures and precautions taken by the hospitals as per the guidelines, fastening of any liability on the hospital would be peculiarly difficult.
The defence available to the hospital may be culpability and negligence of the employee and proving that the hospital itself took all possible measures to avoid any mass spread of the infection.
The next relevant point to be analysed and answered is that when a Non COVID-19 patient contracts the virus during his term of being admitted in the hospital what are the Legal obligations of the hospital when this happens?
The National Consumer Dispute Redressal Commission in the matter of Apollo Emergency Hospital vs Dr. Bommakanti Sai Krishna & Anr.[6] observed that “As already observed, the infection occurred during the stay of the Complainant at the hospital. On the other hand, there is nothing to show that the source of infection lay outside the hospital. Thus, there is preponderance of possibilities of the infection having been acquired in the hospital itself. We therefore, do not accept the contention that it was necessary for the Complainant to produce expert evidence to prove negligence on the part of the concerned doctors in the hospital.”
The afore-stated judgement implies a presumption of liability on the hospital that in cases where the probability of acquiring the infection is much higher inside the hospital than from other sources. However, the same may not apply in COVID cases in light of the peculiar difficulty of tracing the source of acquiring the COVID-19 infection. Therefore, the presumption rendered by the aforesaid judgement will not be ipso facto applicable to cases of COVID patients.
As we have discussed the various pertinent relevant questions another one is that what are the legal obligations of the hospital, if and when a patient is misdiagnosed positive or negative for COVID-19 by the hospital due to a fault in the COVID-19 rapid testing kit (“testing kits”)?
The liability of a hospital in cases of misdiagnosis depends on the methodology of procuring of testing kits. A hospital may procure testing kit either from third party manufacturer or may manufacture them internally i.e. by itself or its subsidiary.
In cases where the misdiagnosis is on account of faulty testing kit procured externally, the hospital cannot be held directly liable as the liability may be shifted upon the manufacturer.
In cases where the misdiagnosis is on account of faulty testing kit is due to testing kits produced internally the hospital may be liable subject to it being proved that the misdiagnosed patient was indeed positive. However, factors such as the success rate of any testing kit not being 100% may have an interplay in determining the liability.
We have to be aware of what are the Legal liability of a hospital in a situation where the hospital discharges a mild/very mild/pre-symptomatic COVID patient to ramp up the capacity for serious COVID-19 patients.
A hospital will not be held liable for a systematic discharge of a mild/very mild/pre-symptomatic/moderate COVID-19 patient as the same is directed by the Central Government. On May 8, 2020, the MoHFW released its revised policy for the discharge of COVID-19 patients.[7] This revised policy provides that hospitals can discharge mild/very mild/pre-symptomatic in accordance with the protocols given therein.
In the earlier advisory[8], COVID-19 patients could be discharged only after chest radiograph clearance, viral clearance in respiratory samples, and if two of the patient’s specimens were negative within a period of 24 hours. The discharged patient would then have to home quarantine themselves in accordance with the revised policy.
So what is the protocol to be followed by a Hospital while disposing of the dead bodies of the COVID-19 patients?
The corpses are a source of infection for healthcare personnel/ other patients and cannot be disposed of by usual methods of disposal and therefore, the MHFW issued guidelines dated March 15, 2020 on dead body management in COVID-19.[9] The guidelines provide inter-alia, the protocol to be followed at the time of removal from the isolation room or area, put in bio-hazard bag and disinfection. Further, all surfaces of the isolation area (floors, bed, railings, side tables, IV stand etc.) should be wiped with 1% Sodium Hypochlorite solution and then it should allow a contact time of 30 minutes, and allow it to air dry as well.
While treating patients infected with the COVID-19 virus, what is the protocol for the treatment?
The All India Institute of Medical Sciences (AIIMS) has issued clinical protocol dated April 21, 2020 for treatment of Covid-19 patients and states such as Madhya Pradesh and Delhi have directed Hospitals and health centres dedicated to treating COVID-19 patients to follow the said clinical protocol.[10]
Treatment must be affordable for all. One must know whether or not there is a standardisation of costs of treatment of a COVID-19 for private hospitals?
Government hospitals are reaching their intake capacities and for that reason COVID-19 patients have been resorting to treatment in private hospitals. While some private hospitals are charging exorbitant amounts as costs of treatment, the same is worrying not just for the patients but also to the insurers.[11]
In a first, the State government of Maharashtra has capped treatment costs in private hospitals for people without medical insurance and for other patients, the capped prices will come into effect once they exhaust their medical insurance cover.[12]
The Hon’ble Gujarat High Court has vide its order dated May 22, 2020 directed the state government to issue a notification making it mandatory for all multi-speciality hospitals private/ corporate hospitals in Ahmedabad and on its outskirts to reserve 50% of their beds (or such other capacity as maybe specified by the state government) for COVID-19 patients.
In view of the same, the Government of Gujarat may come up with similar caps on costs as Maharashtra.[13] The Hon’ble Gujarat High Court also observed that the certain private hospitals authorised by the government to treat COVID-19 patients in Ahmedabad are charging exorbitant fees which is unaffordable for a massive section of the society and directed the state government to ensure that private hospitals do not charge exorbitant fees. [14]
Also in light of the same The Hon’ble Bombay High Court recently directed a charitable hospital to make court deposit of monies in a case pertaining to levy of exorbitant charges for treatment of COVID-19 patients belonging to poor strata of the society despite reserving 20% of its beds for poor and the needy.[15]
‘Intellect’ refers to the creations of the mind. Intellectual Property is a type of intangible property and includes inventions, literary and artistic works, symbols, names and paintings.
Intellectual Property Rights (IPRs) are the Rights granted to the creators of Intellectual Property (IP) by the Government. The nature of IPR is territorial. In any country an IP has to seek protection separately under the relevant laws.
Mechanisms which are Special in nature have been kept in place for various territories in order to provide protection to different types of IPRs. It confers an exclusive right to the inventor/ creator or assignee to fully utilize the invention/ creation for a given period of time.
It’s been established that the intellectual labor associated with the innovation should be given due importance so that public good emanates from it.
This is a strong tool, to protect investments, time, money, effort invested by the inventor/creator of an IP, since it grants the inventor/creator an exclusive right for a certain period of time for use of his invention/creation.
Hence it aids in the economic development of a country by promoting healthy competition and encouraging industrial development which shall also aid in the growth of the economy.
WHAT IS AN INTELLECTUAL PROPERTY?
Intellectual Property(IP) refers to creations of the mind; inventions; literary and artistic works; and symbols, names and images used in commerce.
IP is divided into two categories: 1) Industrial Property:- includes patents for inventions,trademarks, industrial designs and geographical indications. 2) Copyright:- covers literary works (such as novels,poems and plays), films, music, artistic works (e.g., drawings, paintings, photographs and sculptures) and architectural design.
In Intellectual property(IP), there are Rights which relates to the rights of performing artists in their performances, producers of phonograms in their recordings, and broadcasters in their radio and television programs are included.
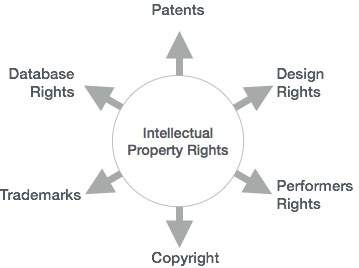
WHAT ARE INTELLECTUAL PROPERTY RIGHTS?
So what do you mean by intellectual property rights? IP rights like any other property right allow creators, or owners, of patents, trademarks or copyrighted works to benefit from their own work or investment in a creation.
These rights are outlined in Article 27 of the UDHR which provides for the right to benefit from the protection of moral and material interests resulting from authorship of scientific, literary or artistic productions.
The importance of intellectual property was first recognized in the Paris Convention for the Protection of Industrial Property (1883) and the Berne Convention for the Protection of Literary and Artistic Works (1886). Both treaties are administered by the World Intellectual Property Organization (WIPO).
There are various pros which are more compelling than the cons.
1) The progress and well-being of humanity rest on its capacity to create and invent new works in the areas of technology and culture.
2) The legal protection of new creations and this encourages the commitment of additional resources for further innovation.
And Lastly the third pros is that the 3) Promotion and protection of intellectual property spurs economic growth, creates new jobs and industries, and enhances the quality and enjoyment of life.
An efficient and equitable intellectual property system can help all countries to realize intellectual property’s potential as a catalyst for economic development and social and cultural well-being. The intellectual property system helps strike a balance between the interests of innovators and the public interest, providing an environment in which creativity and invention can flourish.
INTELLECTUAL PROPERTY HOLDERS IN A QUANDARY DUE TO COVID-19 PANDEMIC
While experts are in a combat mode and the race is on to discover the cure for COVID-19, the claim of intellectual property rights for exclusive use of the cure poses a dilemma as it is not considered the most rational thing to do at the moment.
Carlos Correa addressed to organizations like WHO, WTO and WIPO via an open letter to seek support for WTO countries that invoke the ‘security exception’ contained in Article 73 of the Agreement on Trade Related Intellectual Property Rights (TRIPS) Agreement, to take ‘actions it considers necessary for the protection of its essential ‘security interests’ in the wake of COVID-19 threat.
It has been suggested that invocation of exception under Article 73 will be warranted to procure medical products and devices or to use the technologies to manufacture them as necessary to take cue of the present public health emergency.
By suspending the enforcement of any Intellectual Property right as given under Article 73(b) of TRIPS Agreement, an obstacle for the procurement or local manufacturing of the medical equipments shall be necessary in order to protect the population of the world will be outlasted.
The question which is raised due to the above is regarding IP rights which are aimed to aid the public by promoting technological advancement in return of providing the inventor an exclusive right over the invention, though for a limited time. Though the IP rights are at a standstill due to the outbreak the IP Registry offices all over have limited their functioning.
TYPES OF INTELLECTUAL PROPERTY
Trade Mark: –
A trademark is used in order to identify a business entity and it also differentiates the goods made or services offered by a company or an individual. Names, Words, Logos, Colors, Packaging, Sounds (audible), Signs (visual) or any combination thereof are considered and can be filed as trademarks.
A trademark must be Unique and Distinctive in nature and must also avoid adjectives for eg efficient and Names of person or places (E.g. India). Even Obscene words, Religious or Government words or symbols (E.g. OM) and Common Shapes (Square) should be avoided.
The Trade mark means a mark used in relation to goods for the purpose of indicating a connection in the course of trade between the goods and some person having the right as proprietor to use that mark.
The function of a trade mark is to give an indication to the purchaser or a possible purchaser as to the manufacture or quality of the goods, to give an indication to the trade source from which the goods come or the trade hands through which they pass on their way to the market.
The Trade Marks Act, 1999 is an act which provides for the registration and better protection of trademarks for goods and services and for the prevention of the use of fraudulent marks. A trade mark is valid for a period of 10 years.
Case Name: The Coca-Cola Company v. Bisleri International Pvt. Ltd Case Citation: Manu/DE/2698/2009
Copyright: –
Copyright is an exclusive legal right granted to the creators of an intellectual work. The owner of a Copyright has rights to reproduce, translate, adapt, perform, distribute and must be publicly allowed to display the work, etc.
Registration is not mandatory since copyright comes into existence as soon as the intellectual work is created but it is recommended to register a copyright for better enforceability, since registered copyrights have more evidentiary value in court.
(a) Types of Works covered under Copyright:-
(1) Literary including Software – Books, Essay, Compilations, Computer Programs.
(2) Artistic – Drawing, Painting, Logo, Map, Chart, Plan, Photographs, Work of Architecture.
(3) Dramatic – Screenplay, Drama.
(4) Musical – Musical Notations.
(5) Sound Recording – Compact Disc.
(6) Cinematograph Films – Visual Recording which includes sound recording.
(b) Duration of Copyright:-
(1) Literary, Dramatic, Musical or Artistic Works – Lifetime of the author + 60 years from the death of the author.
(2) Anonymous & Pseudonymous Works – 60 years from the year the work was first published.
(3) Works of Public Undertakings & Government Works – 60 years from the year the work was first published.
(4) Works of International Organizations – 60 years from the year the work was first published.
(5) Sound Recording – 60 years from the year in which the recording was published.
(6) Cinematograph Films – 60 years from the year in which the film was published.
Case Name:- Indian Performing Rights Society Ltd. v. Eastern India Motion Picture Association Case Citation: – 1977 SCR (3) 206
Designs: – The Design Act, 2000 states that it protects the aesthetic and ornamental features of an object. As per the Act a 2D or 3D pattern of a handicraft, a product, or even an industrial commodity.
The Unique Selling Point (USP), protects the looks and feels of the product and it prevents the duplication of the product. An industrial design helps in drawing a customer’s attention and helps in increasing the commercial value of an article.
Case Name:-Cello Household Products v. M/S Modware India and anr Case Citation:- Notice of Motion (L) No. 209/2017 in Suit (L) No. 48/2017
Patents On the 4th December, 2018, The Ministry of Commerce and Industry released the draft (rules amendment) for Patents Act 1970. These rules are mainly amended with respect to international applications, patent opposition and a few form related extensions. The Central Government proposes to make these amendments in exercise of the powers conferred by section 159 of the Patents Act, 1970.In order to align with TRIPS, inventions which are not patentable have been included even, wider rights of patentee is incorporated. Uniform period of protection is 20years. Case Name: Bajaj Auto Limited v.TVS Motor Company Limited. Case Citation: JT 2009 (12) SC 103
5. Integrated Circuits
Semiconductor Integrated Circuits Layout Design (SICLD) Act 2000 states the meaning of Semi conductor Integrated Circuit as, a product having transistors and other circuitry elements designed to perform an electronic circuitry function. There are 2 types of designs as per the act:-
(i) Layout Design – A layout of transistors and other circuitry elements including lead wires which connects semiconductor integrated circuits.
(ii) Layout-Design Registry (SICLDR) is the office where the applications on Layout-Designs of integrated circuits are filed for registration. The jurisdiction of this Registry is whole of India. The Registry, as per the guidelines laid down in the Semiconductor Integrated Circuits Layout Design (SICLD) Act 2000 and the Semiconductor Integrated Circuits Layout-Design (SICLD) Rules 2001, examines the layout-designs of the Integrated Circuits and issues the Registration Certificate to the original layout-designs of the Semiconductor Integrated Circuits.
Case Name: Sunil Alag v. Union of India and Others Case Citation: W.P. (C) 8152/2013
6. Biological Diversity
The Biological Diversity Act 2002 was enacted to realize the objectives enshrined in the United Nations Convention on Biological Diversity (CBD) 1992 which was passed by the Lok Sabha on 2nd December 2002 and by the Rajya Sabha on 11th December 2002.
It recognizes the sovereign rights of states to use their own Biological Resources due to the scarcity and also to conserve it. The Act provides for a mechanism for equal sharing of benefits arising out of the use of traditional biological resources and knowledge. It is a federal legislation enacted by the Parliament of India for preservation of biological diversity in India.
Case Name: Environment Support Group vs National Biodiversity Authority Case Citation: W.P. No.41532 / 2012
7. Plant Varieties and Farmers
Protection of Plant Varieties and Farmer’s Rights Act of 2001(PPV & FR Act, 2001) confers right to breeders, researchers and farmers over their plant varieties. Reaching legislation with regards to establishing rights for farmers to save, use, exchange and sell farm saved seed.
The Act establishes nine rights for farmers of which the most important in this regard are the right to “seed” and the right to “compensation” for crop failure (Art. 39). Not only does the 2001 Act protect the rights of framers to save, use, exchange and sell farm- saved seed, it also seeks to ensure that these seeds are of good quality, or at least that farmers are adequately informed about the quality of seed they buy.
In addition, safeguards are provided against innocent infringement by farmers. Farmers who unknowingly violate the rights of a breeder are not to be punished if they can prove that they were not aware of the existence of such a breeder’s right (Art 42).
Case Name:- Monsanto Technology LLC & Ors Vs. Nuziveedu Seeds Ltd & OrsHigh Court of Delhi Case Citation: CS (Comm) 132/2016
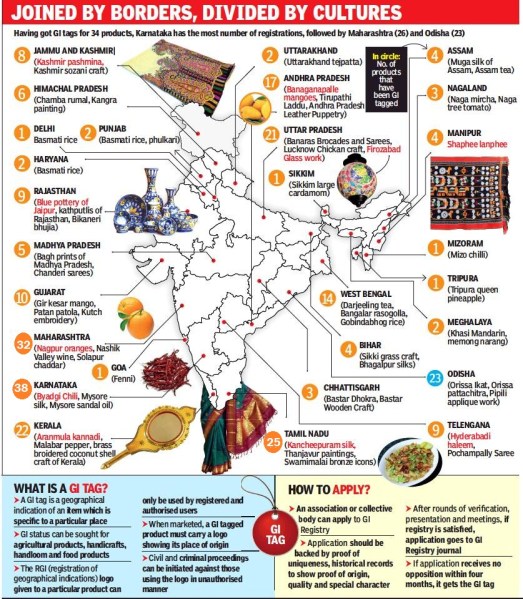
The Geographical Indication of Goods:- The Geographical Indications of Goods (Registration and Protection) Act, 1999 states Geographical Indication as it is primarily an agricultural or food product, natural or a manufactured product (handicrafts, Handloom textiles or industrial goods) originating from a definite geographical territory. A product is considered to be manufactured in a territory if any one of the activities of either the production or of processing or preparation of the goods takes place there. It promotes the producers prosperity of goods which have been produced in the geographical territory.
It helps the producer community to differentiate its products from other competing products that are present in the market and generate goodwill around its products. Hence, it acts as a signaling device by helping consumers to identify genuine quality products.
Case Name:- Tea Board Vs ITC Limited on 20 April, 2011 Case Citation:- GA No. 3137 of 2010 CS No. 250 of 2010
It has been suggested that invocation of exception under Article 73 will be warranted to procure medical products and devices or to use the technologies to manufacture them as necessary to take cue of the present public health emergency.
CONCUSION
The above overview clearly depicts that India has adopted and adhered to the latest IPR Regime and it has forayed into the global trade competition with a double edged sword.
Individual defensive gear (PPE) — face veils and shields, gloves, head and shoe spreads, and hazardous materials suits — is apparently left flung at the incineration grounds. This is a general wellbeing and ecological danger, particularly with regards to Covid-19. Point by point standards for the correct removal of the PPE were set up by the Central Pollution Control Board (CPCB) as ahead of schedule as late March. The zenith contamination control body must guarantee that these standards are followed and those spurning them face substantial fines.
PPE has been named biomedical waste. Given the infectious idea of the ailment and the fluctuating life expectancy of the infection, the CPCB concluded that, notwithstanding the Biomedical Waste Management Rules, the removal of PPEs required a lot of explicit standards, including the way of assortment, bundling for transport (twofold layer of pressing to dodge spillage) and removal. These standards are authoritative on medicinal services offices, isolate and segregation focuses, living arrangements in instances of home consideration, test assortment focuses and research centers, urban bodies and their substances, for example, incineration and cemetery, and the basic biomedical waste treatment offices. The guidelines are point by point, and whenever followed ought to take into account sheltered and appropriate removal of PPEs.
Usage has reliably been the Achilles heel . Before the Covid-19 pandemic, India produced approximately 550 tons of biomedical waste each day yet rebelliousness was uncontrolled. Human services offices neglected to isolate the waste and didn’t pay expenses for normal biomedical waste treatment offices. Covid-19 has intensified consistence The CPCB and its state units, in association with state governments, must advance up implementation and punish the individuals who bomb the standards. Ill-advised waste removal will just exasperate the circumstance.
There has been lot of pressure on police force in such hard times especially in Maharashtra which is worst hit state in India.In the wake of this crisis, state government has decided to recruit as many as 10,000 new police constables to make situations under control. This is very crucial decision taken by government as state is now seeing huge surge in active corona cases. There are now 2 lakh 17 thousand case in the state with almost 10,000 deaths. Nearly 6-10 thousands new cases are seen per day.
According to an official statement, the decision was taken during a meeting presided over by Pawar at the Mantralaya, which was attended by state Home Minister Anil Deshmukh and senior officials.
“A decision has been taken to recruit 10,000 personnel in the police shipai (constable) category to strengthen law and order in the state and reduce work stress on the force,” the statement quoted Pawar as saying.
A meeting had taken place under the chairmanship of Ajit Pawar in which these two decisions were taken by the committee comprises of state’s Home Minister Anil Deshmukh, Additional Chief Secretary (Home) Sitaram Kunte, Additional Chief Secretary of Finance department Manoj Saumik and other concern officials of Home & Revenue department. Maharashtra Police DIG Subodh Jaiswal and SRPF’s Additional DG Archana Tyagi were present in the meeting.
The decision will help youths from urban and rural areas to serve for the country. The recruitment process will be conducted without violating social distancing norms. The process is assured to be completed till the year end.
Moreover, 1,384 posts can be created within the ladies’s battalion and the recruitment can be accomplished in three phases, by filling 461 posts in every stage, the deputy chief minister mentioned within the assertion.


















You must be logged in to post a comment.