The HSTDV is an unmanned scramjet demonstration aircraft for hypersonic speed flight. It is being developed as a carrier vehicle for hypersonic and long-range cruise missiles, and will have multiple civilian applications including the launching of small satellites at low cost. The HSTDV program is run by the Indian Defence Research and Development Organisation. India is pushing ahead with the development of ground and flight test hardware as part of an ambitious plan for a hypersonic cruise missile.
The Defense Research and Development Laboratory’s Hypersonic Technology Demonstrator Vehicle (HSTDV) is intended to attain autonomous scramjet flight for 20 seconds, using a solid rocket launch booster. The research will also inform India’s interest in reusable launch vehicles. The eventual target is to reach Mach 6 at an altitude of 32.5 km (20 miles).
India is pushing ahead with the development of ground and flight test hardware as part of an ambitious plan for a hypersonic cruise missile. The Defense Research and Development Laboratory’s Hypersonic Technology Demonstrator Vehicle (HSTDV) is intended to attain autonomous scramjet flight for 20 seconds, using a solid rocket launch booster. The research will also inform India’s interest in reusable launch vehicles. The eventual target is to reach Mach 6 at an altitude of 32.5 km (20 miles).
Initial flight testing is aimed at validating the aerodynamics of the air vehicle, as well as its thermal properties and scramjet engine performance. A mock-up of the HSTDV was shown at the Aero India exhibition in Bangalore in February (see photo), and S. Panneerselvam, the DRDL’s project director, says engineers aim to begin flight testing a full-scale air-breathing model powered by a 1,300-lb.-thrust scramjet engine in near future.
Future strike: When when ready for test and subsequent use, the hypersonic missiles will considerably augment India’s arsenal, putting it along a a handful of countries that have such weapons. Besides the velocity of over five times the speed of sound (Mach 5), the manoeuvring capability of hypersonic missiles makes maximum very effective offensive weapons capable of defeating enemy missile defence and tracking systems.A Hypersonic missile’s potency is the speed at which it travels, enabling it to have a quick reaction time considered invaluable for both defence and offence.
India has been working on making BrahMos – a supersonic cruise missile – hypersonic and the scramjet will help in the endeavour too. Developed jointly with Russia, the BrahMos now files at Mach 2.8 speed.
Low cost sat launches Further, on the civilian side, the HSTDV can total satellites at low cost. However, its ability to do so will be restricted. Experts believe that such a vehicle using scramjet can only push satellites into LEO (LOW EARTH ORBIT), and the air breathing engines will not find oxygen at higher altitudes.
According to ISRO, at present, satellites are launched by multistage satellite launch vehicles that can be used only once (expendable). these launch vehicles carry oxidizer along with the fuel for combustion to produce thrust. large vehicles design for one time use are expensive and their efficiency is low because they can carry only 2-4 % of their lift off mass to orbit.
Nearly 70% of the propellant (fuel oxidizer combination) carried by today’s launch vehicles consists of oxidizers. Therefore, the next generation launch vehicles must use a propulsion system which can utilise the atmospheric oxygen during their flight through the atmosphere which will considerably reduced the total propellant and required to place a satellite in orbit. Also, if those vehicles are made reusable, the cost of launching satellites will further come down significantly. Thus, the future reusable launch vehicle concept along with air breathing propulsion is an exciting candidate offering routine access to space at a far lower cost.
A- Sat Capabilities
A Hypersonic vehicle/missile also has the potential to augment India’s anti satellite (A-Sat) capabilities. The country, on March 27 2019, successful be conducted an A-Sat missile test in an operation codenamed ‘Mission Shakti’, making it only the fourth country after the US China and Russia to demonstrate such a capability.
Development is a multi-dimensional phenomenon. Some of its major dimensions include: the level of economic growth, level of education, level of health services, degree of modernization, status of women, level of nutrition, quality of housing, distribution of goods and services, and access to communication. In India, the progress of socio-economic development among major states is not uniform. This study examines the existing variability of inter-state development and thereby identifying the indicators responsible for the diversity in development. Instead of studying the variability of a particular variable across states, a composite index based on several indicators has been developed using principal component analysis and states are arranged according to the indices derived using four broadly accepted components: (a) economic production and economic condition or in other words level of economic development; (b) common minimum needs; (c) health and health-related services and (d) communication. The findings of the analysis support the general perception about the states. The states in India are marked with wide disparity in socio-economic development. The factors, which are found out to be more important for the overall development process, relate to basic needs like education, availability of food, minimum purchasing power and facilities like safe drinking water, health care infrastructure, etc. It is also found that enrolment ratio cannot be raised unless minimum needs of the common people are satisfied. Therefore, true development requires government action to improve elementary education, safe drinking water facilities and health care, and to remove barriers against social minorities, especially women. The role of social development such as literacy (and particularly of female literacy) in promoting basic capabilities emerges as the prerequisite to overall development.
These results clearly emphasize the role of well-functioning public actions in improving the overall living conditions of the people. Although economic growth in the sense of expanding gross national product and other related variables is one of the most fundamental input to the overall development process, the basic objective of development should focus on the expansion of human capabilities which has been neglected for long in India.
By 2030, 40% of Indians will be urban residents. However, there will also be more than 5,000 small urban towns (50,000-100,000 persons each) and more than 50,000 developed rural towns (5,000-10,000 persons each) with similar income profiles, where aspirations are fast converging with those of urban India. The figure below illustrates urban-rural population distribution in India in 2005, 2018, and 2030 projected. Three critical “access” barriers currently constrain the aspirations of those living in rural areas in India. First, constrained physical connectivity ; second, lack of digital connectivity ; and third, limited financial inclusion. While incomes may have begun to rise in rural India, this may not translate into commensurate growth of productivity and inclusion, unless the urban-rural divides are reduced. Given the approximately 60% share of rural population in 2030, this is a critical imperative not only for the government, which serves its people, but also for businesses which are looking for new opportunities and new growth markets in India. A high priority is infrastructure development, both physical and digital, to enable rural dwellers to access the products and services matching their incomes, needs and aspirations. The government already has flagship programmes such as Digital India, which envisions transforming the country into a digitally empowered society and knowledge economy centred on key programme pillars, such as broadband connectivity and universal access to mobile connectivity, and professed roles, such as “faceless, paperless, cashless”. With sustained, efficient execution, such innovative programmes in digital and financial areas, along with the proposed improvement of physical infrastructure (road connectivity to nearby urban centres and reliable power supply to all rural households), will be key drivers to ensure inclusive growth in India, truly bridging urban-rural divides across multiple levels.
Various factors, such as the level of literacy, female education, nutritional standards, infant mortality, morbidity, employment, income distribution, public distribution system, political commitments etc., and their corresponding interactions, contribute to these striking variations among states inn the livelihood of common people. It may be mentioned that broad state-level comparison may not be able to capture fully the extent of diversities among various indicators characterizing several facets of development. Nevertheless, state-level indicators are of prime importance as far as the state is a crucial and political unit. A wide range of relevant fields of actions, including health and education, are constitutionally defined as ‘state subjects’, to be handled by the individual states rather than the central government, or as ‘concurrent subjects’, involving both state and central governments.
Biomedical Waste Management & Handling Rules, 1998 (“1998 Rules”) in India govern the handling, disposal and management of bio-medical waste (“BM Waste”)in India have been notified by the Central Government in the exercise of the powers conferred by Section 6,8 & 25 of the Environmental Protection Act, 1986. These rules provide for the framework of the management and Handling of disposal and scientific management of BM Waste
In wake of the COVID-19 pandemic, the Centre Pollution Control Board (“CPCB”) recently issued guidelines dated March 27, 2020 for handling, treatment and safe disposal of BM Waste generated during treatment, diagnosis and quarantine of patients confirmed or suspected to have COVID-19 (“Guidelines”).
The Guidelines have been necessitated due to the super infectious nature of the Novel corona virus and provide for a mechanism for the segregation, packaging, transportation, storage and disposal of BM Waste in order to avoid further spread of the virus through BM Waste.
So what do you mean by the BM Waste and what are the categories of BM Waste that the hospitals generate?
The Bio-Medical Waste Management Rules 2016[1] (“2016 Rules”) define the BM Waste as any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or research activities pertaining thereto or in the production or testing of biological or in health camps, including the categories mentioned in Schedule I the 2016 Rules.
The 2016 Rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form. The next imminent question that comes to our minds is what are the categories of BM Waste that the hospitals generate?
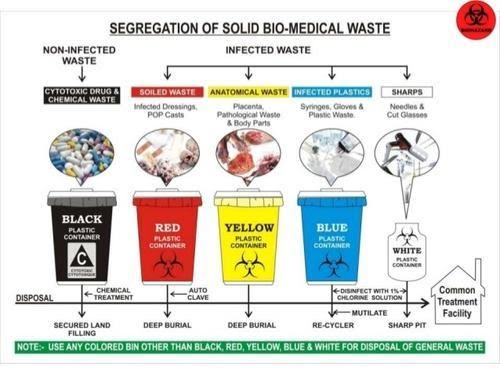
BM Waste generated from a hospital could be human anatomical waste, animal waste- microbiology & biotechnology, waste sharps, discarded medicines and cytotoxic drugs, solid & liquid waste.
Now that we know what’s the meaning and various categories of BM Waste, the most pertinent question arises that how is it supposed to be treated and disposed of by the hospitals in India during the ongoing COVID-19 pandemic?
While the hospitals in their usual course deal with the segregation, management and storage of BM Waste, the situation in times of COVID-19 is extraordinary the reason being the highly contagious nature of the virus and also it’s transmission cycle and multiplicity rate.
As the hospitals are being flooded with the suspected and confirmed cases, the Ministry of Health and family welfare (“MoHFW”) and the CPCB have issued various guidelines for the handling and management of waste generated from the COVID-19 facilities.
Under the 2016 Rules, while the hospitals are required to ensure that there is a secured location within its premises for a spill/pilferage free storage of segregated BM Waste in labelled/coloured bags or containers, the duty to transport the stored BM Waste from the hospital premises onwards to the common BM Waste treatment and disposal facility is of an ‘operator’ as defined in the Rules.
Specifically, in wake of COVID-19, the CPCB has issued Revision 1 to the Guidelines dated March 25, 2020 for Handling, Treatment and Disposal of Waste Generated during Treatment/Diagnosis/ Quarantine of COVID-19 Patients (“CPCB Guidelines”).
[2] The said CPCB Guidelines inter-alia, state that hospitals are required to depute separate BM Waste sanitation workers to COVID-19 isolation wards and maintain records of all waste generated in such isolation wards and ensure that the BWM generated is collected and separately stored in separate leakproof color-coded double layered bags or bins /containers labelled as “COVID-19 waste” as per the 1998 Rules and the Guidelines.
In fact the Bombay High Court in a recent pending public interest litigation has, while issuing notices to local municipal corporations and the State Pollution Control Board, also directed the Maharashtra government to clarify whether it was ensuring that all COVID-19 related biomedical waste generated in the state was being disposed of in a safe manner[3].
Now that we have a thorough understanding of how the BM Waste is supposed to be treated and disposed of the most important and the widely discussed about topic is that what are the measures that a hospital is required to take for the safety of its employees doctors, nurses and other support staff who are known as the (“healthcare personnel”) from the dangerous diseases like COVID-19?
In order to answer this pertinent question which is often there in the limelight, one must keep in mind that the Healthcare personnel who are the Frontline workers have a high risk of contracting the COVID-19.
While the hospitals are taking precautions and measures to control any spread of infection within the premises, it is particularly difficult given the highly super-infectious nature and hyper-speed feature of the virus. Due to this feature it spreads widely and it becomes a bit difficult to contain it in an over-crowded environment but it’s not impossible to achieve that as we all have been deterrent enough to contain it’s spread but still there is always scope for improvement.
The first steps towards controlling the spread of a virus is personal protective equipment also known as PPE which should preferably be a two-layered fluid-resistant apron and basic items like N-95 masks, face shield, full cover gowns and sanitisers but the same are rendered ineffective against the COVID-19 if the quality of these equipments is not up to the standard as required.
Greater emphasis is also to be laid upon the proper training and awareness of healthcare personnel towards proper use and disposal of the equipment. The spread of the COVID-19 virus is also particularly fast due to the heavy load of asymptomatic patients coming into the hospital and hence a greater need for the formulation of national COVID-19 protocol.
The MoHFW has vide its revised guidelines for clinical management of COVID-19 dated March 31, 2020[4] (“Clinical Management Guidelines”) impressed upon strict compliance of Infection prevention control (IPC) protocol for Hospitals and a consequent effect of the same is prevention and management of COVID-19 in the hospital staff.
This protocol inter-alia, standard precautions such as hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin, prevention of needle-stick or sharps injury, safe waste management, cleaning and disinfection of equipment and cleaning of the environment around a COVID-19 patient.
The 2016 Rules also provide as follows that in order to and for ensuring the safety of the healthcare workers and others involved in the segregation and pre-treatment of BM Waste, the hospital is required to train to all its healthcare workers, immunise them for protection against diseases which likely to be transmitted by handling of BM Waste, in the manner as prescribed in the National Immunisation Policy[5].
Also, hospitals are required to ensure occupational safety of all its health care workers and others involved in handling of BM Waste by providing appropriate and adequate PPE and also they must conduct health check ups at the time of induction and at least once in a year maintain the records for the same.
Now due to the pandemic if one is an employee ie the Healthcare personnel of the hospital one must understand the Legal aspect and angle also and the most important aspect of all is that what is the Legal obligations of the hospital, if and when an employee of the hospital tests positive for COVID-19.
Let’s answer this as it’s the most crucial and critical aspect. The present COVID-19 pandemic is an unprecedented event and is unlike any other infectious disease known to mankind and the medical world which is yet to fully decipher its modus operandi of infecting humans.
In a hypothetical situation wherein a hospital employee contracts COVID-19, it will be imperative for the employee in such a situation to establish that his possible exposure to COVID-19 was in the Hospital itself not in the community after considering that the employee is spending time outside as well apart from the hospital premises.
While in an ideal case, if it is proved that a hospital staff has contracted it ,i.e., it shall amount to ‘a hospital acquired infection’, then the hospital would be ordinarily liable. However, in the case of COVID-19 since it is seemingly impossible to trace down the exact source of the infection, in absence of such evidence and in light of utmost safety measures and precautions taken by the hospitals as per the guidelines, fastening of any liability on the hospital would be peculiarly difficult.
The defence available to the hospital may be culpability and negligence of the employee and proving that the hospital itself took all possible measures to avoid any mass spread of the infection.
The next relevant point to be analysed and answered is that when a Non COVID-19 patient contracts the virus during his term of being admitted in the hospital what are the Legal obligations of the hospital when this happens?
The National Consumer Dispute Redressal Commission in the matter of Apollo Emergency Hospital vs Dr. Bommakanti Sai Krishna & Anr.[6] observed that “As already observed, the infection occurred during the stay of the Complainant at the hospital. On the other hand, there is nothing to show that the source of infection lay outside the hospital. Thus, there is preponderance of possibilities of the infection having been acquired in the hospital itself. We therefore, do not accept the contention that it was necessary for the Complainant to produce expert evidence to prove negligence on the part of the concerned doctors in the hospital.”
The afore-stated judgement implies a presumption of liability on the hospital that in cases where the probability of acquiring the infection is much higher inside the hospital than from other sources. However, the same may not apply in COVID cases in light of the peculiar difficulty of tracing the source of acquiring the COVID-19 infection. Therefore, the presumption rendered by the aforesaid judgement will not be ipso facto applicable to cases of COVID patients.
As we have discussed the various pertinent relevant questions another one is that what are the legal obligations of the hospital, if and when a patient is misdiagnosed positive or negative for COVID-19 by the hospital due to a fault in the COVID-19 rapid testing kit (“testing kits”)?
The liability of a hospital in cases of misdiagnosis depends on the methodology of procuring of testing kits. A hospital may procure testing kit either from third party manufacturer or may manufacture them internally i.e. by itself or its subsidiary.
In cases where the misdiagnosis is on account of faulty testing kit procured externally, the hospital cannot be held directly liable as the liability may be shifted upon the manufacturer.
In cases where the misdiagnosis is on account of faulty testing kit is due to testing kits produced internally the hospital may be liable subject to it being proved that the misdiagnosed patient was indeed positive. However, factors such as the success rate of any testing kit not being 100% may have an interplay in determining the liability.
We have to be aware of what are the Legal liability of a hospital in a situation where the hospital discharges a mild/very mild/pre-symptomatic COVID patient to ramp up the capacity for serious COVID-19 patients.
A hospital will not be held liable for a systematic discharge of a mild/very mild/pre-symptomatic/moderate COVID-19 patient as the same is directed by the Central Government. On May 8, 2020, the MoHFW released its revised policy for the discharge of COVID-19 patients.[7] This revised policy provides that hospitals can discharge mild/very mild/pre-symptomatic in accordance with the protocols given therein.
In the earlier advisory[8], COVID-19 patients could be discharged only after chest radiograph clearance, viral clearance in respiratory samples, and if two of the patient’s specimens were negative within a period of 24 hours. The discharged patient would then have to home quarantine themselves in accordance with the revised policy.
So what is the protocol to be followed by a Hospital while disposing of the dead bodies of the COVID-19 patients?
The corpses are a source of infection for healthcare personnel/ other patients and cannot be disposed of by usual methods of disposal and therefore, the MHFW issued guidelines dated March 15, 2020 on dead body management in COVID-19.[9] The guidelines provide inter-alia, the protocol to be followed at the time of removal from the isolation room or area, put in bio-hazard bag and disinfection. Further, all surfaces of the isolation area (floors, bed, railings, side tables, IV stand etc.) should be wiped with 1% Sodium Hypochlorite solution and then it should allow a contact time of 30 minutes, and allow it to air dry as well.
While treating patients infected with the COVID-19 virus, what is the protocol for the treatment?
The All India Institute of Medical Sciences (AIIMS) has issued clinical protocol dated April 21, 2020 for treatment of Covid-19 patients and states such as Madhya Pradesh and Delhi have directed Hospitals and health centres dedicated to treating COVID-19 patients to follow the said clinical protocol.[10]
Treatment must be affordable for all. One must know whether or not there is a standardisation of costs of treatment of a COVID-19 for private hospitals?
Government hospitals are reaching their intake capacities and for that reason COVID-19 patients have been resorting to treatment in private hospitals. While some private hospitals are charging exorbitant amounts as costs of treatment, the same is worrying not just for the patients but also to the insurers.[11]
In a first, the State government of Maharashtra has capped treatment costs in private hospitals for people without medical insurance and for other patients, the capped prices will come into effect once they exhaust their medical insurance cover.[12]
The Hon’ble Gujarat High Court has vide its order dated May 22, 2020 directed the state government to issue a notification making it mandatory for all multi-speciality hospitals private/ corporate hospitals in Ahmedabad and on its outskirts to reserve 50% of their beds (or such other capacity as maybe specified by the state government) for COVID-19 patients.
In view of the same, the Government of Gujarat may come up with similar caps on costs as Maharashtra.[13] The Hon’ble Gujarat High Court also observed that the certain private hospitals authorised by the government to treat COVID-19 patients in Ahmedabad are charging exorbitant fees which is unaffordable for a massive section of the society and directed the state government to ensure that private hospitals do not charge exorbitant fees. [14]
Also in light of the same The Hon’ble Bombay High Court recently directed a charitable hospital to make court deposit of monies in a case pertaining to levy of exorbitant charges for treatment of COVID-19 patients belonging to poor strata of the society despite reserving 20% of its beds for poor and the needy.[15]
In amidst this global pandemic,life has become very harsh for many poor and middle class people. This lockdown has also locked the earnings making them struggle everyday to meet their daily needs. The biggest question of the hour has turned out to be”when will this pandemic meet an end?”.But it is necessary that we must focus on life after corona.
This corona virus has taught us many things ,it has helped in integration of people not only in the country but also worldwide. This virus has taught us that discrimination of people on basis of caste,religion,region has no sense. It has also became agent of mother earth wherein it brought the pollution levels significantly down all over the world.
It is clear indication that we must start using non-conventional energy sources after this crisis. It is clear that we must understand that humanity is the only religion and serving needy is next to serving god.
We should maintain social distancing at least for following year and help needy. If we all stand United and act wisely we will surely be victorious in this situation and once again we can live that golden days enjoying railway rides, shouting for our favourite team in stadiums and the birds chirping in the forest without our intervention, but for now we must stay home stay safe.






You must be logged in to post a comment.