One of the most important products of global addiction demand is an alcoholic beverage. In developing countries like India, alcohol consumption tends to be a major problem because of the various socio-cultural practices across the nation, different alcohol policies and practices across the various states, lack of awareness of alcohol-related problems among the community, false mass media propaganda about alcohol use, various alcohol drinking patterns among the alcohol consumers and the emergence of social drinking as a habit because of the widespread urbanisation across the country.
Social consequences of alcohol use
Alcohol consumption not only affects the individuals but also his family members get affected in one way or the other. The person in an intoxicated state may indulge in domestic violence with his family members; may exhaust the savings of the family, which can negatively affect the education of his children, and the children of alcoholic fathers will have strained relationship with their family members, which can affect their psychological wellbeing.
Road traffic accidents
One of the major problem of alcohol consumption are road traffic accidents which occur due to driving vehicles under the influence of alcoholic beverages. Both developing and developed countries report high rates of road traffic accidents because of alcohol consumption.
Primary care intervention for alcohol-related problems
In developing countries like India, primary care physicians are the first contact of patients with the healthcare system. primary care management of alcohol-related problems include three core steps, namely, counselling the patient on the ill-effects of alcohol and, if necessary, prescribing medications like disulfiram and connecting with the patients by organizing treatment programs and forming support groups. If necessary, they have to refer the patient to higher centres for further care and management.
BUT WHAT ABOUT PEOPLE WHO CAN’T AFFORD THESE TREATMENT AND SUFFERES FROM ITS CONSEQUENCES
In many countries AA Meetings are held for being a support emotionally and spiritually to an alcoholic person with no financial support and most of all countries it being held have not only they have accepted this but hole heartedly supported it some for their family members or some for their friends suffering from alcoholism.
What is AA?
Alcoholics Anonymous is a fellowship of men and women who share their experience, strength and hope with each other that they may solve their common problem and help others to recover from alcoholism.
The only requirement for membership is a desire to stop drinking. There are no dues or fees for AA membership; we are self-supporting through our own contributions. AA is not allied with any sect, denomination, politics, organization or institution; does not wish to engage in any controversy; neither endorses nor opposes any causes. Our primary purpose is to stay sober and help other alcoholics to achieve sobriety.
AA is nonprofessional – it doesn’t have clinics, doctors, counsellors or psychologists. All members are themselves recovering from alcoholism. There is no central authority controlling how AA groups operate. It is up to the members of each group to decide what they do. However, the AA program of recovery has proved to be so successful that almost every group follows it in very similar ways.
WHAT DOES A.A. DO?
A.A. members share their experience with anyone seeking help with a drinking problem; they give person-to-person service or “sponsorship” to the alcoholic coming to A.A. from any source.
The A.A. programme, set forth in our Twelve Steps, offers the alcoholic a way to develop a satisfying life without alcohol.
HISTORY OF AA IN INDIA
Here is an account of how AA came to India and it’s growth in the subsequent years. Though there are no accurate records from the early days, what is definitely clear is that Harold M., a school teacher by profession, was the first person in India, to stop drinking and gain lasting sobriety through the spiritual principles of Alcoholics Anonymous. He stopped drinking on 5th May 1957, and hence that date is nationally acknowledged as the “Founders Day” in India.
On 5th May 2021, AA completed 64 years of its service in India. Looking back, the results are heart-warming. The wide support and awareness generated by the groups in India and its members inspires immense hope for the future.
AWARENESS OF AA
In India, AA meeting is a program which mostly seen by people through foreign movies and shows not through advertisement or medical portals as its necessity seems nonsensical by people especially in India because of their traditional values about alcohol where some drinks it as a medicine and some as men for showing their authority and masculinity over others, stupid norms like that make bad habit like drinking into ADDICTION.
Histoplasmosis is a fungal infection caused by Histoplasma capsulatum, a fungus. Spores suspended in the air by birds and bats are frequently the source of this illness. If the infection is limited to the lungs, it is not dangerous. It might be deadly if it spreads across the entire body. This condition mostly affects immune-compromised people, most of who are suffering from AIDS.
Histoplasma capsulatum is a soil microorganism that is frequently linked with decomposing sediments. Infectious elements are frequently released by disrupted soil particles, which are breathed by humans and settle into their lungs.
Histoplasmosis is often known as the Darlings’ disease, after Samuel Darling, who first found the virus in Panama.
SYMPTOMS
Histoplasmosis is characterised by a high fever. The fungus Histoplasma causes no symptoms in the majority of persons who are exposed to it. Others may experience symptoms that subside on their own. Coughing: Fatigue (severe exhaustion): Chills: Headache: Body aches: Chest pain Histoplasmosis symptoms might emerge anywhere from 3-17 days after a person inhales the fungus spores. These symptoms usually fade away in a few weeks to a month for most people. However, some people’s symptoms might persist much longer, particularly if the condition is acute. Histoplasmosis can cause a long-term infection in certain individuals, especially those with compromised immune systems, or it can move from the lungs to other regions of the body, such as the central nervous system.
RISK AND PREVENTION
If you’ve been in a region where Histoplasma is present in the environment, you can acquire Histoplasmosis. It I s frequently linked to soil disturbance, specifically soil containing bird and bat droppings. Certain persons are more likely to acquire severe types than others:
People who have weakened immune systems, for example, people who:
Are patients of HIV/AIDS
Had an organ transplant
Are taking medications such as corticosteroids or TNF-inhibitors
Infants
Adults aged 55 and older
Histoplasmosis cannot be transmitted from one person to another or between humans and animals through the lungs. The illness can, however, be transferred through a transplant with an affected organ in exceedingly rare circumstances.
In regions where it is prevalent, it might be difficult to avoid breathing it in. People with compromised immune systems should avoid undertaking behaviours that are known to be linked with Histoplasmosis in locations where it is present, such as:
Disturbing material where there are bird and bat droppings
Cleaning chicken coops
Exploring caves
Cleaning, remodelling, and tearing down old buildings
Professional firms that specialise in the cleaning of hazardous material should clear up large volumes of bird and bat droppings.
TREATMENT AND DIAGONOSIS
Although direct diagnosis of Histoplasmosis (HP), one of the most common endemic mycoses in the world, is achieved by micro as well as macroscopic observation of Histoplasma capsulatum, serologic indication of this infection is important because etiologic agent isolation is time-consuming and unresponsive. To identify specific antibodies to H. capsulatum, a number of immunoassays have been utilised. Immuno-diffusion is the most often used technique for antibody detection, with a sensitivity of 70 -100 percent depending on the clinical form.
The complement fixation test, which was formerly widely employed, is less specific (60 – 90 percent). Immunoassays for detecting fungal antigens are particularly useful in patients with low immunity, with positive predicted results of 96–98%. The majority of modern diagnostic tests still use unpurified antigenic complexes derived from entire fungal cells or their culture filtrates. Clinical immunoassays employing highly pure and well-characterized antigens, including recombinant antigens, are now the focus.
For diagnosis doctors use your medical and travel history, symptoms, physical examinations, and laboratory testing. Taking a blood sample or a urine sample and submitting it to a facility is the most frequent way that healthcare practitioners test for Histoplasmosis.
Imaging studies, such as chest X-Rays or CT scans of lungs may be performed by your healthcare professional. A sample of fluid from your lungs is used or a tissue biopsy is performed, which involves taking a tiny sample of damaged tissue from your body and examining it under a microscope. Research facilities may also examine if Histoplasma may develop in bodily fluids or tissues.
Symptoms may go away without therapy in some persons. To treat severe infection in the lungs, persistent Histoplasmosis, and infections that have moved from the lungs to other areas of the body, prescription antifungal medicine is required. Antifungal medications like Itraconazole are widely used to treat Histoplasmosis. If you have a minor case treatment is typically not required. However, if your symptoms are severe, or if you have the chronic or disseminated type of the condition, you’ll almost certainly need antifungal medication. You may need to take medicines for three months to a year if you have a severe version of the condition.
The avoidance of apoptosis by cancer cells is a prominent characteristic of cancer. Since apoptosis inhibition is at the heart of tumour growth, the clearing of malignant cells and retaining a definite number of healthy cells involves tumour-cell death. Cellular death pathway targeting provides some possible therapeutic targets for all cancers. The most obvious strategy for cancer treatment is to concentrate on lesions, particularly apoptosis in tumour cells, which eliminate cell death.
Apoptosis is an essential component of normal development. For keeping normal physiological processes between cell proliferation and cell deaths, homeostatic balance is essential. Aberrant control of apoptotic mechanisms is one of the main characteristics of cancer growth and development. Apoptosis can be activated by triggering two different molecular pathways, a pathway of the extrinsic, a death receptor or a mitochondrial pathway, intrinsic pathway also called apoptotic cascade. Extrinsic pathways from outside the cells are activated by pro-apoptotic receptors, such as CD95 and TNF-related ligands inducing apoptosis (TRAIL) interacting with specialised cell surface death receptors. Mitochondrial (intrinsic) pathways induce the transcription of or the post-translational activation of BH3 proapoptotic B-cell leukaemia / lymphoma 2 (Bcl-2) family proteins from the inside of the cell, as a result of extreme cell pressure such as DNA or cytoskeleton damaging apoptotic protease-activating factor-1 (Apaf-1) and assemblies of Cytochrome c activate caspase 9. This caspase activates the effector 3, 6 and 7 caspases, which perform apoptosis. Latest development of different therapeutic methods that interfere with apoptosis and are commonly used or studied for cancer treatment are becoming popular. It induces cancer cell death or enhances the response to certain cytotoxic medicines of cancer cells and CCs. Some of them are still in preclinical and clinical trials such as caspase activators, apoptosis modulators or agents targeting apoptosis-related proteins. Future methods for targeting apoptotic pathways in cancer patients with promising application are also seen.
Therapeutically inducing apoptosis strategies
The progressive pre-clinical or early clinical development of many therapeutic approaches inducing apoptosis are seen. The research processes two styles from a mechanical perspective of separate approach: (a) specifically separating tactics induce apoptosis, which is here called pro-apoptotic; and (b) survival-signalling techniques that modulate this to promote apoptosis, which is called permissive approach.
Proapoptotic approach:
Apoptin. A promising tumour killing technique
Apoptin (VP3) is a cell used when sparing normal cells and killing only tumour cells. The chicken anaemia virus is a source of 14,000 proteins. Latest evidence shows that this molecule induces apoptosis in which Caspases are included. Apoptin is very much shown, in vitro findings, that it is active against cancer cells without induction of natural toxicity Cells. The basic effect of it being this tumour killing only could be clarified by nuclear tumour cell location of the protein, activity requirement, whereas the protein in normal cells are Cytoplasm localised. In addition, apoptin is also active and potentially chemo resistant in genetically disrupted cells such as p53, Bcl-2 or tumour cells that express BCR-ABL. Apoptin is under progress in tumour cells in vivo in gene therapy strategies. Multiple injections of adenovirus into healthy rats or nude mouse have not been found toxic in preclinical studies. Furthermore, antitumor effects in the nude s.c. mouse were observed, hepatoma in human beings. These findings, however, remain preliminary and more preclinical work is needed with human cells to ensure safety and evaluate apoptin ‘s potential as an anti-cancer compound better.
Apoptosis was examined for the development and treatment of cancer by attempting to determine its function in chemotherapy cytotoxicity caused by agents. Cytotoxic agents frequently lead to apoptotic by only a fraction of the cells. A significant portion of cells must be recruited into apoptosis to allow maximum use of apoptosis as a mechanism for anti-neoplastic agent response. The only regularly used cytotoxic agents that have been shown to induce apoptosis in breast cancer cells are paclitaxel (Taxol ®). Another of such cytotoxic agents is cyclophosphamide, and furthermore cytosine arabinoside is also used. Quantitative measurements of apoptotic cells were performed by controlling the binding of the phosphatidylserine-binding protein (FITC)-labelled annexin V into cellular cells.
Inhibitor of apoptosis protein (IAP)
The genome of baculoviruses was the original founder of IAPs because of their capacity in infected host cells to inhibit apoptosis. Re-based on the survival and XIAP of recent attempts to use IAPs to obtain anti-cancer treatment. In vitro experiments showed that the anti-apoptotic function of the proteins was inhibited by caspases-3, -7, and -9. As these cases have shown to be important in vitro for chemical apoptosis aimed at its natural inhibitors, the IAPs have been identified as a possible means of increasing chemosensitivity. In fact, NSCLC cells inhibited up to 70 per cent of surviving mRNA expression with the use of the oligonucleotide 4003, resulting in etoposide sensitization of cancer cells. Additionally, the downregulation of XIAP in ovarian cancer cells with wild type p53 by adenoviral antisense expression has caused apoptosis. These promising findings have led to clinical trials using anti-sense IAPs being mapped. The IAPs’ function may be more complex than the in vitro data initially suggested. Indeed, in NSCLC patients c-IAP1, c-IAP2, and XIAP had no precedented response to chemotherapy responses, unlike most of the expected multiple in vitro trials. Moreover, in patients with non-Hodgkin’s lymphoma and AML, there were no variations in reaction to chemical therapy between survivin-positive and negative instances. Furthermore, XIAP expression was not associated and did not have any relation with the apoptotic index of NSCLC patients but was inversely related to tumour growth. In this group of patients, higher XIAP expression has been predictively converted into a considerably longer overall survival. In addition, the nuclear localisation of survivor has shown positive effects on prognosis in a recent study of gastric cancer patients. These findings verified that it may mean that limitless ODN survival inhibition may not be desirable both within the cytoplasm and the nucleus. It is possible that the IAPs are engaged in apoptosis inhibition by the blocking of caspase but also other essential functions including proliferating. These conflicting results can be clarified. In addition, the net effect of IAPs can depend on their interaction with the control molecules Smac / DIABLO, HtrA2 and Factor1 associated with XIAP, an antagonist of the XIAP apoptotic operation. Therefore, while it is potentially promising, additional functional research and IAP interactions are required to better utilise them as goals for anti-cancer therapy.
BH3 Mimetics
There is a common consensus that BH3-only proteins are essential for apoptosis, promulgating inherent and extrinsic pathways of cell death. Based on the blocks of the sequence homology called BH domains, proapoptotic members from the BCL-2 family may be further identified. Only one domain, in general called the α-helical BH3 region is available for all BH3 protein. This preserved BH3 domain played a key role in the treatment of cancer. Three BCL-2 protein subgroups: BH3 (BCL-2 homology 3), BCL-2, BCL-2-associated X-protein (BAX), and the BCL-2 antagonist-killer (BAK), interacting on one another on the mitochondrial membrane, activate the pathway. This is the basis of three distinct groups. BH3-only proteins have been shown to achieve two mechanisms by transmitting signals to induce apoptosis, and only BH3-proteins inducted by transcriptional or post-translational cytotoxic stress. The neutralisation of antiapoptotic BCL-2 proteins or direct activation of BAK and BAX 47 is a clear way to understand the previous mode of action, both structurally and functionally, and hence the goal for production of pharmaceuticals. By attaching its hydrophobic groove by adding four hydrophobe residues it antagonises the BCL-2 antiapoptotic protein family members. Members such as cell-death antagonist BCL-2 and NOxa bind to their anti-apoptotic brothers, while other proteins such as BIM, tBID and PUMA only neutralise other anti-apoptotic agents.
miRNA
The miRNAs (MiRNAs) is a small endogenous class of 18 to 25 nucleotide length non-encoding RNAs which modify gene expression by mRNA degradation or mRNA deletion. The mature-miRNA products are produced by sequential processing by the ribonucleases Drosha and Dicer1 from a longer primary miRNA (pri-miRNA) transcript. miRNAs are known to inhibit thousands of target genes, since the objective mRNA needs only partial complementarity. Thus, one miRNA can target at the same time to a complexity of mRNAs, and several miRNAs can control the expression of one particular mRNA. The alteration of miRNAs includes a varying variety of human diseases, including cancer, by natural mechanisms miRNA are involved in number of process, including cell growth, differentiating, proliferating, apoptosis, and stem cells self-renovation. The de-regulation of miRNA also induces apoptosis avoidance, involving tumorigenesis and pharmaceutical resistance. The functioning of aberrated miRNAs, which are closely linked to the apoptosis mechanism, will act as oncogenes (OncomiRs) or tumour suppressors (TSmiRs) during tumour induction and progression. Manipulation of the levels of miRNA expression affecting apoptosis genes and pathways may also be a clinical approach to develop successful cancer treatment. Furthermore, because cancer cells frequently display a distinct trend for miRNA expression, novel profiles of altered miRNA expression may be useful for tumour-diagnosed molecular biomarkers, disease-specific outcome predictions and tumour-aggression evaluations. Therefore, numerous anti-cancer therapies are being designed to recover miRNA behaviours and rebuild gene regulation networks or drug sensitivity. A number of miRNAs were associated with drug resistance, some of them linked to apoptosis. Deregulation of miR-214 is a frequent phenomenon in ovarian cancer in human beings and it has been shown that miR-214 mainly targets PTEN / Akt pathways and promotes cell survival and cisplatin tolerance. It’s also recognised that the let-7 miR family plays an essential part in a number of cellular functions including opioid sensitivity modulation. The miRNA let-7a, aimed at caspase-3 in human cancers, was over-expressed and demonstrated resistance to a range of drugs, including doxorubicin, paclitaxel and interferon-gamma, which are caspase-3-dependent. Let-7e was up-regulated with improved tolerance to doxorubicin in some ovary cancer cell lines. Conversely, let-7i has been documented as uncontrolled in ovarian cancer resistant to chemotherapy, and the reintroduction of let-7i could sensitise ovarian resistant cell line to platinum-based chemotherapy. The cause of apoptosis induced by the chemo preventive agent curcumin has been shown to be the downregulation of miR-185 in a non-small cell-lung cancer cell line which increased its direct target expression, Caspase-10. The effect on miRNA expression profiles was thus studied by anti-cancer drugs that modulate apoptosis cell proliferation and could help predict the resistance to apoptosis. This will help prevent needless morbidity and represent a new class of biomarks to allow customised care through the awareness of possible miRNAs involved in apoptosis resistance.
Blebbishield Formation
The development of blebbishields is one method used by cancer stem cells to resist apoptosis. The emergency system is enabled to rescue the stem cells in apoptotic cancer. The apoptotic blebs merge together into a formed sphere called blebbishields. Cells undergoing blebbishield development display visual symptoms of apoptosis, but the reaction is prevented and ends in cells living. Serpentine filopodia formation due to endocytosis are involved in blebbishield formation to avoid complete apoptotic reaction. Apoptosis normally results in secondary necrosis from a lack of ATP, blebbishields by activating glycolysis are able to prevent secondary necrosis. In order to ensure clinical effectiveness, cancer stem cells must be blocked to survive in parallel to treatments by apoptosis. A variety of possible candidates were identified including inhibitors of caspase, Smac mimetics and inhibitors of the translation at an internal ribosome entrance site (IRES). IRES translation is regulated by antiapoptotic proteins, such as cIAP-2, and XIAP. IRES translation facilitates survival by converting the cIAP-2, which enflames the mechanism and moves the antiapoptotic to the proapoptotic equilibrium towards antiapoptotic survival. Hemming IRES translation will prevent blebbishield formation from being started. N-Myc is an IRES translation goal intended to avoid the development of blebbishield.
Conclusion
Apoptotic approach to seeking alternative anti-cancer drugs is intriguing, since it is not unique to the form of cancer. In both the extrinsic and intrinsic pathways of cancer there are various mutations that cause cells to evade apoptosis, which is a distinctive characteristic of cancer. A more general cancer cure will also include the opportunity to target and activate apoptotic tract. Many compounds extracted from plants that are not toxic to healthy cells are particularly promising compounds to cause apoptosis.
An ancient and quiet honourable practise has been the use of preventive medicine. For example, the ancient Chinese use to pay their doctors while they remained healthy, however as soon as they felt sick this payment would not be given. The effectiveness of antibiotics as a prophylactic means for protecting healthy individuals exposed to pathogenic bacteria, preventing the development of an infection in chronically ill patients and preventing an infection in patients who undergo surgery is a debatable issue. Many surgeons reported significant reductions in post-operative infection following antibiotic use, and a few did not even reported infections for a period of twenty years. Despite this success, prophylaxis presents certain hazards, including the evolution of antibiotic resistance, superinfections and drug side effects, for the individual patient and for the general public. Therefore, physicians have broad views on the responsible preventive use of antibiotics. However, antimicrobial prophylaxis (AP) should be confined to specific well-accepted evidence for the prevention of excess costs, toxicity and antimicrobial resistance in order to effectively prevent infections. Initial or secondary (recurring prevention or reactivating infections) prophylaxis may also be regarded as primary (prevention of initial infections) or may be administered to prevent infection by killing a colonising organism. Patients should know in detail the potential risks and benefits of AP. The potential risks are allergic reactions with the use of antibacterial agents that can be serious or life-threatening, and clostridium difficile colitis. The risk of tendinitis, including the rupture of the tendon of Achilles should be alerted to patients taking fluoroquinolones.
The pros and cons of using antimicrobials as a prophylactic.
THE PROS: In the diagnosis of life-threatening acute bacterial infections, surgical infectious diseases and if there is an effective use of antimicrobials as prophylaxis, antibiotics can have many benefits.
In bacterial infections: In acute bacterial infections, which were highly mortal before introduction of antibiotics, the benefits of antibiotics as prophylactics is most clearly indicated. Mortality in endocarditis was about 100% prior to 1990 and about 20% total in 2010 although the death rate is usually caused not by unsuccessful antibiotic therapy but by cardiac failure or embolic complications. In bacterial meningitis in 1990, the mortality rate was reduced to 8% to 20% in 2010 and acute osteomyelitis mortality decreased from 50% to less than 1%. Many other infections, in both individual patients and others within the community, have significantly reduced morbidity and serious effects of spraying. In high-risk patients, this included the use of antibiotic prophylaxis for bacterial meningitis. During the systemic inflammatory response (SIR) stage of the infection, the early initiation of broad- spectrum antibiotics was proved critical for preventing the development of sepsis. When appropriate antibiotics are prescribed early in the surgical sepsis, mortality is significantly reduced.
In surgical site infections: Although the technique is still less than good surgical and aseptic technique, the risk of surgical site infection is considerably decreased by antibiotic prophylaxis in high-risk surgical patients such as operations over 2 hours, abdominal procedures, endogenous or exogenous contamination and co-morbidity. The choice of antibiotics depends on the organisms that are most likely to be affected; the kind of operation; the probability of resistance development and the financial cost involved. In felines, the rate of postoperative infections was reduced in the course of the optional orthopaedic surgery by preoperative antibiotic prophylaxis. Therefore, it is usually advisable to treat routine perioperative prophylactic antibiotics, even if numerous orthopaedic operations are categorised as clean. Orthopaedic procedures normally last longer than 90 minutes and the potential infection may be influenced by local wound factors like implants and tissue trauma. In the presence of implants, bone and joint infections are very difficult to treat, increase morbidity and may adversely affect the result. Cefazolin is currently seen as a choice antibiotic because of its outstanding effectiveness, low toxicity and reasonable costs against most surgical wound pathogens. The first dose should be given at a concentration of 22 mg/kg 30–60 minutes before surgery. The dose is usually recommended to be repeated every 90–120 minutes, but there is evidence that the frequency is enough every three hours.
The selection criteria of the antibiotic are:
The most prone bacteria that could cause infection should be identified. A prophylactic against frequently found skin bacteria (skin flora) is used when only an incision in the skin is made. An antibiotic is chosen to treat both the skin and the mucosal flora if the mucosal incision is involved.
Chemical and drug toxicity characteristics.
The least likely antibiotic that is required for serious infections is chosen if different antibiotics are equally helpful for prophylaxis. This helps prevent antibiotic resistance from developing.
Sensitivities specific to the environment of the specific hospital. Some hospitals may be very frequent with methicillin-resistant infections, while vancomycin or clindamycin-resistant infections in other hospitals may be more frequent.
CONS: The drawbacks of prophylactic antimicrobials are shown by side effects, resistance development and opportunistic pathogens.
Side effects: Their ability to cause serious or fatal adverse reactions sometimes provides a reason to limit the use of antibiotic agents for true therapeutic indications. For example, the most commonly used antibiotics for UTI prevention are nitrofurantoin, trimethoprim/sulfamethoxazole (TMP / SMX), but these drugs have negative reactions in children. Gastrointestinal disturbance, skin reactions such as urticaria, maculopapular rash are the common adverse reactions to nitrofurantoin. Almost exclusively because of sulfamethoxazole, most commonly dermal, adverse events related to trimethoprim/sulfamethoxazole. Serious side effects are extremely rare and mostly reversible when treatment is discontinued but they do exist. The long-term use of low-dose urinary prophylaxis antibiotics is therefore not completely safe. While adverse reactions existed in children to these medications, the lower dose of prevention and the lack of significant co-morbidities and medicinal interactions in children are much less common in children than in adults. In 1% of patients, penicillin causes death from type I anaphylactic shock in sensitive allergic patients and have other harmful consequences. High dose of penicillin may be associated with serum sickness (type III reaction), penicillin, thrombocytopenia, and haemolytic anaemia from cytotoxic antibodies. There is 10 percent cross-sensitivity between the derivatives of penicillin, cephalosporin and carbapenems because they share a similarity between the side chain rather than the beta-lactam structure. Therefore, the same or closely related drug must be avoided to which the patient has shown sensitivity in the past. In certain circumstances, certain drugs are more likely to be toxic. Ampicillin and amoxicillin rash are more common when lymphoid tissue is ebullient, in the case of lymphomas or glandular fever. The following are commonly used antimicrobials for prophylaxis along with their side effects:
Penicillin: side effects are reactions of hypersensitivity, renal damage, low potassium (hypokalemia)
Cephalosporin: side effects are reactions of hypersensitivity, reduction of blood cell levels such as: neutrophils, leucocytes (leucopoenia) and thrombocytopenia, nausea and vomiting, gastrointestinal problems diarrhoea, anorexia.
Metronidazole: side effects are toxicity of the CNS, problems in gastrointestinal tract, neutropenia, blood clotting problems, and alcohol reactions
Antibiotic resistant: The bacterial resistance mechanisms are known to include genetic changes, antibiotic metabolism by bacteria, like beta lactamase (beta lactamases), altered receptor site affinity, cell wall permeability alterations (antibiotic efflux pump) and the environmental influence at infection sites. In pus, most bacteria are relatively resistant in the dormant phase. The slow cellular immune mechanism does not affect the intracellular microbes such as tubercle bacillus, Brucella abortus, and Salmonella typhi. This partly explains the slowness of antibiotics in these infections. Infections on heart valves and the meninges, for example, are more resistant to antibiotics than infections elsewhere because the concentrations of polymorphs and macrophages are low. Inappropriate antibiotic treatment facilitates the spread of resistance. In many countries, UTI-associated antibiotic resistance has become widespread. Previous studies showed an increased rate of antibiotic resistance. Antimicrobial resistance in enteric and oropharyngeal flora may be developed through the use of antibiotics for prophylaxis. A recent study has reported a high rate of resistance against third generation cephalosporins in children who received prophylactic antibiotics. Clinicians are advised to carefully use prophylactic antibiotics. Additional hazards are present in antibiotics that inhibit the growth of a range of different types of bacteria. These medications also eliminate benign bacteria that help protect us from diseases by competing with pathogenic bacteria and limiting their propagation. Wide ranging antibiotics may produce deep changes in bacterial population composition and lead to the outgrowth and invasion of so-called superinfections of antibiotic-resistant strains.
Since the V. Cholerae infection dose is high, proper hygiene generally makes immunisation and prophylaxis unnecessary, hence antimicrobial prophylaxis in endemic areas has not proved effective. In the prevention of sexually transmitted diseases, chemical prophylaxis is ineffective. The use of antimicrobials to prevent genital diseases may, indeed, deteriorate the situation by selecting harder resistant strains. Antibiotic products, especially those of a wide activity range, alter the normal flora of the body, allowing resistant and opportunistic pathogens to colonise and multiply. These could cause secondary infections in a healthy female, such as candida vaginitis, or fungal and systemic infection in a highly susceptible patient, such as an immunosuppressive treatment. Clostridium difficile, anaerobic bacterium which can multiply after normal flora is suppressed and is relatively resistant to many commonly employed antibiotics but metronidazole or vanzomycin, causes the severe complication of pseudomembraneous colitis. Between 2000 and 2007, 400 percent of the increased mortality from Clostridium difficile infection was partially due to the emergence of the insusceptible C. fluoroquinolone strain. When pseudomembraneous colitis is developed in transplant patient, it is impaired to absorb the immunosuppressive medications which increase allograft-rejection susceptibility.
Other disadvantages of prophylactic use of antimicrobials are:
More expensive treatment: Antibiotics are costly and shouldn’t be used inappropriately. However, the cost of the antibiotics is negligible compared to the cost of hospitalisation for a long stay due to a wound infection in patients at clearly reduced risk of wound infections which were found by prophylaxis. The least cost-effective agent for a short period of time is selected if antibiotic prophylaxis is used.
Allergies and toxic reactions: When antibiotics are used, toxic or allergic reactions may occur. These can be reduced for brief periods by using safe agents.
The use of antibiotics can lead to a false sense of safety. Careful surgery and precautionary and postoperative care are essential if wound infections are to be minimised.
Infection due to side effects by drugs, especially clindamycin, with bacteria such as the Clostridium difficile.
Conclusion:
The use of antimicrobial prophylaxis has led to a large number of infections being prevented and significant declines in surgical infections at the site. Specific, accepted indications should be limited to antimicrobial prophylaxis to avoid excess cost, toxicity and resistance to antimicrobials. The potential risks and benefits of any antimicrobial prophylaxis system should be understood by patients. Although there is evidence based antimicrobial prophylaxis practises, many are based on low evidence or expert advice. Additional antimicrobial prophylaxis studies are necessary. There remain significant controversies in antimicrobial prophylaxis, with many opportunities to practise improvement through rigorous studies. More antibiotics do not always reduce surgical site infection more effectively. There are significant gaps between directives and practises, mainly over the current guidelines on antibiotic prophylaxis.
A study published in a medical journal has revealed that SARS-CoV-2, which causes Covid-19, has undergone multiple mutations in its “spike proteins”. This is the protein that gives the virus the ability to infiltrate the human cells. Once this occurs, the virus starts replicating, which leads to infection.
The paper published in Journal of Laboratory Physicians was based on an analysis of 1,604 spike proteins extracted from 1,325 complete genomes and 279 partial spike coding sequences of SARS-CoV-2 available at National Center for Biotechnology Information (NCBI) in the US till May 1.
Dr Sarman Singh, the lead author of the study, said they found 12 mutations in the spike proteins, six of which were novel mutations. “One deletion was also found in an Indian strain (MT012098.1). Deletion means change in the genetic structure of the virus. We don’t know how it will affect the virulence of the disease though,” he added.
The maximum genetic mutations were observed in spike proteins extracted from genomes of SARS-CoV-2 from the US, the experts said. “Viruses are known to mutate or change their genetic structure upon exposure to different environments. But in this case, the change is happening quite fast. We are not sure how it will affect the disease spread,” Singh said.
The others participants of the study included experts from Infectious Diseases and Immunity in Global Health Programme, Research Institute of McGill University Health Center, and McGill International TB Center, Canada. The study said spike protein was the major target for vaccine development, but several mutations were predicted in the antigenic epitopes across all genomes available globally.
“The emergence of various mutations within a short period might result in conformational changes in the protein structure, which suggests that developing a universal vaccine could be a challenging task,” the study added. Mutation was also found in the antigens responsible for producing antibodies, indicating that the patients infected with the mutants would have very low or nil antibodies.
Recently, Hong Kong reported a case of re-infection due to Covid-19. Similar cases have also been documented in the US and India. “Even if a person gets Covid-19 again due to a mutated strain of the virus, the likelihood of severe symptoms would be less as seen in the patient in Hong Kong. This is because the antibodies against one strain of Covid-19 can offer protection against the mutated virus too. However, further scientific study and analysis is needed to ascertain this. The disease is new and we are still learning about it,” said a virologist from Maulana Azad Medical College.
In Delhi, the cases of Covid-19 had dipped significantly in July. However, it has started rising over the past few days. While lack of social discipline and opening of the economy are two key factors, many doctors said a mutation of the virus could also be behind it. “Multiple strains of the virus have been identified in the country, including the original one from Wuhan, China and the ones spreading in Europe,” said a doctor. The World Health Organization does not expect widespread vaccinations against COVID-19 until the middle of next year, said a spokeswomen, stressing the importance of rigorous checks on their effectiveness and safety.
The emergency use approval authorisation by US Food and Drug Administration (US FDA) to use plasma as a potential therapy for Covid in US is expected to provide impetus to its used as yet ‘promising’ treatment option in India, even as doctors say clear scientific evidence is needed.
The US President announced US FDA approval on August 23, though the agency put it on hold over doubts on it’ efficiency. Doctors claim that the therapy of using recovered Covid-19 patients plasma to treat infected people will get even more widespread in India, given the endorsement from US. This would be similar to the sharp surge in demand witnessed for anti-malarial drug hydroxychloroquine as a potential covid 19 treatment, after President Trump’s repeated backing and later failed in global trials.
US FDA previously issued an EUA to allow hydroxychloroquine sulfate and chloroquine phosphate donated to the Strategic National Stockpile (SNS)to be distributed and used for hospitalized Covid-19 patients. In fact, these two drugs have been used for decades for the therapy and control of malaria and autoimmune diseases.
Preliminary studies have suggested HUQ may have utility in fighting covid-19. Distinct possible effects may be selected to its function in the treatment of covid-19 patients : A. anti-virus, B. anti-inflammation and C. anti-thronebotic. As until now there have been no data indicating HCQ has any immunity boosting effect, here we will mainly discuss the anti-virus and anti-inflammation effects. Both CQ and HCQ have been shown to possess anti-viral activity against various viruses such as human immunodeficiency virus (HIV), hepatitis A virus, hepatitis C virus, influenza A and B viruses, influenza A HSNI virus and others. Recent studies reported that CQ and HCQ could also inhibit SARS-CoV-2 in vitro, suggesting that they are potentially applicable to Covid-19 patients. However, there is to date no convincing report of the in viro anti-viral effects of HCQ/CQ. Several randomized controlled trials brought comforting news that CQ and HCQ showed potential effects in reducing respiratory symptoms and pulmonary inflammation as evaluated by computed tomography (CT) of covid 19 patients. It led to panic buying as people attempted to acquire this purpoted ” life saving drug”. Even some physicians stocked up CQ and HCQ for personal use in US and some European countries.
One person in US died and another become seriously ill after using verterinary formulation of CQ tablets intended for use in fish tanks in an effort to present Covid-19. Shortly after permitting the use of CQ and HCQ for treating covid-19, the US FDA issued precautions on using those drugs. Hence, we believe that serious discussions of the potential mechanisms are urgently needed to guide the potential clinical application, evaluation of efficacy and prevention of adverse effects of these drugs.
Plasma therapy has become the most common and simple treatment used niw-a-days in Covid-19 treatment. The US FDA announced that convalescent plasma may be effective in treating covid-19 and potential benefits of the product outweigh the risks based on scientific evidence available.
In India, multi-centre clinical trials to study whether plasma therapy is a useful covid-19 treatment are underway by the Indian Council of Medical Research. Further, States like Maharashtra are running the world’s largest plasma therapy trials, Project Platina, in 18 medical colleges, but response from donars reportedly has been lackluster. Covid therapy is highly individualised. The use of plasma therapy can be life-saving in certain cases and is being used in compassionate grounds. It is a promising treatment option if used earlier in the cycle of the disease. It has been used as therapy for over 100 years, but for COVID-19, we need to document this in a research programme. We also need better methodology for its use while screening donors so as to know the adequate level of neutralizing antibody, ortiters”, told Dr.Shashanka Josh.
Significantly, World Health Organisation on Monday remaind cautious about endorsing the use of plasma to treat infected people. “The results are not conclusive”, its chief scientist Soumya Swaminathan said’ adding ” We recommend that convalescent plasma is still and experimental therapy, and should be continued to be evaluated in well-designed randomised clinical trials.”
The US FDA decision was based on an observational study that gave “some positive signals that convalescent plasma can be helpful in treating COVID-19” and might reduce the mortality if administered early after diagnosis. This article is posted on preprint service and is yet to find its way into a medical journal. However, the claims made by the US FDA commissioner have considerably done more harm to the science and raised unrealistic hopes among the public.
In India, plasma is being promoted asking people to donate plasma to save lives, and shaming COVID-19 survivors who chose not to donate. We seem to have accepted plasma therapy widely without any good quality evidence supporting its use. This is likely to give even more widespread with the endorsement from the US, said Dr.Lancelot Pinto consultant respirologist at Mumbai-based PD Hinduja Hospital.
Plasma reduces death rates if there are enough neutralizing antibodies in the donor plasma. As of now, our labs are not accurately measuring the titres of antibodies in donor plasma – thus it is a wild guess if plasma administered to the COVID patient would indeed benefit the patients”, Kalantri added.
US FDA’s statement implies a 35% absolute improvement in outcomes, when the reality is a 32% improvement and that two comparing early late plasma, Dr.Pramesh said, adding, the danger of such a public statement is that ongoing randomised trials of convalescent plasma will struggle to recruit patient. However, the US FDA still recommend that randomised trials of plasma continue.
Biomedical Waste Management & Handling Rules, 1998 (“1998 Rules”) in India govern the handling, disposal and management of bio-medical waste (“BM Waste”)in India have been notified by the Central Government in the exercise of the powers conferred by Section 6,8 & 25 of the Environmental Protection Act, 1986. These rules provide for the framework of the management and Handling of disposal and scientific management of BM Waste
In wake of the COVID-19 pandemic, the Centre Pollution Control Board (“CPCB”) recently issued guidelines dated March 27, 2020 for handling, treatment and safe disposal of BM Waste generated during treatment, diagnosis and quarantine of patients confirmed or suspected to have COVID-19 (“Guidelines”).
The Guidelines have been necessitated due to the super infectious nature of the Novel corona virus and provide for a mechanism for the segregation, packaging, transportation, storage and disposal of BM Waste in order to avoid further spread of the virus through BM Waste.
So what do you mean by the BM Waste and what are the categories of BM Waste that the hospitals generate?
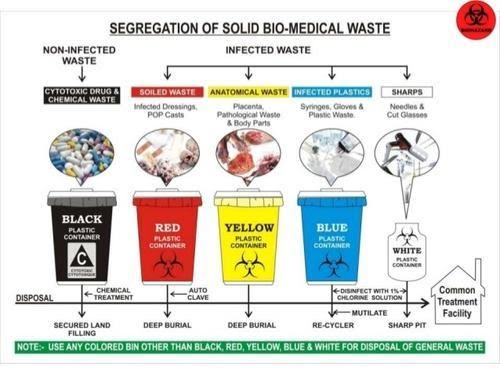
The Bio-Medical Waste Management Rules 2016[1] (“2016 Rules”) define the BM Waste as any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or research activities pertaining thereto or in the production or testing of biological or in health camps, including the categories mentioned in Schedule I the 2016 Rules.
The 2016 Rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form. The next imminent question that comes to our minds is what are the categories of BM Waste that the hospitals generate?
BM Waste generated from a hospital could be human anatomical waste, animal waste- microbiology & biotechnology, waste sharps, discarded medicines and cytotoxic drugs, solid & liquid waste.
Now that we know what’s the meaning and various categories of BM Waste, the most pertinent question arises that how is it supposed to be treated and disposed of by the hospitals in India during the ongoing COVID-19 pandemic?
While the hospitals in their usual course deal with the segregation, management and storage of BM Waste, the situation in times of COVID-19 is extraordinary the reason being the highly contagious nature of the virus and also it’s transmission cycle and multiplicity rate.
As the hospitals are being flooded with the suspected and confirmed cases, the Ministry of Health and family welfare (“MoHFW”) and the CPCB have issued various guidelines for the handling and management of waste generated from the COVID-19 facilities.
Under the 2016 Rules, while the hospitals are required to ensure that there is a secured location within its premises for a spill/pilferage free storage of segregated BM Waste in labelled/coloured bags or containers, the duty to transport the stored BM Waste from the hospital premises onwards to the common BM Waste treatment and disposal facility is of an ‘operator’ as defined in the Rules.
Specifically, in wake of COVID-19, the CPCB has issued Revision 1 to the Guidelines dated March 25, 2020 for Handling, Treatment and Disposal of Waste Generated during Treatment/Diagnosis/ Quarantine of COVID-19 Patients (“CPCB Guidelines”).
[2] The said CPCB Guidelines inter-alia, state that hospitals are required to depute separate BM Waste sanitation workers to COVID-19 isolation wards and maintain records of all waste generated in such isolation wards and ensure that the BWM generated is collected and separately stored in separate leakproof color-coded double layered bags or bins /containers labelled as “COVID-19 waste” as per the 1998 Rules and the Guidelines.
In fact the Bombay High Court in a recent pending public interest litigation has, while issuing notices to local municipal corporations and the State Pollution Control Board, also directed the Maharashtra government to clarify whether it was ensuring that all COVID-19 related biomedical waste generated in the state was being disposed of in a safe manner[3].
Now that we have a thorough understanding of how the BM Waste is supposed to be treated and disposed of the most important and the widely discussed about topic is that what are the measures that a hospital is required to take for the safety of its employees doctors, nurses and other support staff who are known as the (“healthcare personnel”) from the dangerous diseases like COVID-19?
In order to answer this pertinent question which is often there in the limelight, one must keep in mind that the Healthcare personnel who are the Frontline workers have a high risk of contracting the COVID-19.
While the hospitals are taking precautions and measures to control any spread of infection within the premises, it is particularly difficult given the highly super-infectious nature and hyper-speed feature of the virus. Due to this feature it spreads widely and it becomes a bit difficult to contain it in an over-crowded environment but it’s not impossible to achieve that as we all have been deterrent enough to contain it’s spread but still there is always scope for improvement.
The first steps towards controlling the spread of a virus is personal protective equipment also known as PPE which should preferably be a two-layered fluid-resistant apron and basic items like N-95 masks, face shield, full cover gowns and sanitisers but the same are rendered ineffective against the COVID-19 if the quality of these equipments is not up to the standard as required.
Greater emphasis is also to be laid upon the proper training and awareness of healthcare personnel towards proper use and disposal of the equipment. The spread of the COVID-19 virus is also particularly fast due to the heavy load of asymptomatic patients coming into the hospital and hence a greater need for the formulation of national COVID-19 protocol.
The MoHFW has vide its revised guidelines for clinical management of COVID-19 dated March 31, 2020[4] (“Clinical Management Guidelines”) impressed upon strict compliance of Infection prevention control (IPC) protocol for Hospitals and a consequent effect of the same is prevention and management of COVID-19 in the hospital staff.
This protocol inter-alia, standard precautions such as hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin, prevention of needle-stick or sharps injury, safe waste management, cleaning and disinfection of equipment and cleaning of the environment around a COVID-19 patient.
The 2016 Rules also provide as follows that in order to and for ensuring the safety of the healthcare workers and others involved in the segregation and pre-treatment of BM Waste, the hospital is required to train to all its healthcare workers, immunise them for protection against diseases which likely to be transmitted by handling of BM Waste, in the manner as prescribed in the National Immunisation Policy[5].
Also, hospitals are required to ensure occupational safety of all its health care workers and others involved in handling of BM Waste by providing appropriate and adequate PPE and also they must conduct health check ups at the time of induction and at least once in a year maintain the records for the same.
Now due to the pandemic if one is an employee ie the Healthcare personnel of the hospital one must understand the Legal aspect and angle also and the most important aspect of all is that what is the Legal obligations of the hospital, if and when an employee of the hospital tests positive for COVID-19.
Let’s answer this as it’s the most crucial and critical aspect. The present COVID-19 pandemic is an unprecedented event and is unlike any other infectious disease known to mankind and the medical world which is yet to fully decipher its modus operandi of infecting humans.
In a hypothetical situation wherein a hospital employee contracts COVID-19, it will be imperative for the employee in such a situation to establish that his possible exposure to COVID-19 was in the Hospital itself not in the community after considering that the employee is spending time outside as well apart from the hospital premises.
While in an ideal case, if it is proved that a hospital staff has contracted it ,i.e., it shall amount to ‘a hospital acquired infection’, then the hospital would be ordinarily liable. However, in the case of COVID-19 since it is seemingly impossible to trace down the exact source of the infection, in absence of such evidence and in light of utmost safety measures and precautions taken by the hospitals as per the guidelines, fastening of any liability on the hospital would be peculiarly difficult.
The defence available to the hospital may be culpability and negligence of the employee and proving that the hospital itself took all possible measures to avoid any mass spread of the infection.
The next relevant point to be analysed and answered is that when a Non COVID-19 patient contracts the virus during his term of being admitted in the hospital what are the Legal obligations of the hospital when this happens?
The National Consumer Dispute Redressal Commission in the matter of Apollo Emergency Hospital vs Dr. Bommakanti Sai Krishna & Anr.[6] observed that “As already observed, the infection occurred during the stay of the Complainant at the hospital. On the other hand, there is nothing to show that the source of infection lay outside the hospital. Thus, there is preponderance of possibilities of the infection having been acquired in the hospital itself. We therefore, do not accept the contention that it was necessary for the Complainant to produce expert evidence to prove negligence on the part of the concerned doctors in the hospital.”
The afore-stated judgement implies a presumption of liability on the hospital that in cases where the probability of acquiring the infection is much higher inside the hospital than from other sources. However, the same may not apply in COVID cases in light of the peculiar difficulty of tracing the source of acquiring the COVID-19 infection. Therefore, the presumption rendered by the aforesaid judgement will not be ipso facto applicable to cases of COVID patients.
As we have discussed the various pertinent relevant questions another one is that what are the legal obligations of the hospital, if and when a patient is misdiagnosed positive or negative for COVID-19 by the hospital due to a fault in the COVID-19 rapid testing kit (“testing kits”)?
The liability of a hospital in cases of misdiagnosis depends on the methodology of procuring of testing kits. A hospital may procure testing kit either from third party manufacturer or may manufacture them internally i.e. by itself or its subsidiary.
In cases where the misdiagnosis is on account of faulty testing kit procured externally, the hospital cannot be held directly liable as the liability may be shifted upon the manufacturer.
In cases where the misdiagnosis is on account of faulty testing kit is due to testing kits produced internally the hospital may be liable subject to it being proved that the misdiagnosed patient was indeed positive. However, factors such as the success rate of any testing kit not being 100% may have an interplay in determining the liability.
We have to be aware of what are the Legal liability of a hospital in a situation where the hospital discharges a mild/very mild/pre-symptomatic COVID patient to ramp up the capacity for serious COVID-19 patients.
A hospital will not be held liable for a systematic discharge of a mild/very mild/pre-symptomatic/moderate COVID-19 patient as the same is directed by the Central Government. On May 8, 2020, the MoHFW released its revised policy for the discharge of COVID-19 patients.[7] This revised policy provides that hospitals can discharge mild/very mild/pre-symptomatic in accordance with the protocols given therein.
In the earlier advisory[8], COVID-19 patients could be discharged only after chest radiograph clearance, viral clearance in respiratory samples, and if two of the patient’s specimens were negative within a period of 24 hours. The discharged patient would then have to home quarantine themselves in accordance with the revised policy.
So what is the protocol to be followed by a Hospital while disposing of the dead bodies of the COVID-19 patients?
The corpses are a source of infection for healthcare personnel/ other patients and cannot be disposed of by usual methods of disposal and therefore, the MHFW issued guidelines dated March 15, 2020 on dead body management in COVID-19.[9] The guidelines provide inter-alia, the protocol to be followed at the time of removal from the isolation room or area, put in bio-hazard bag and disinfection. Further, all surfaces of the isolation area (floors, bed, railings, side tables, IV stand etc.) should be wiped with 1% Sodium Hypochlorite solution and then it should allow a contact time of 30 minutes, and allow it to air dry as well.
While treating patients infected with the COVID-19 virus, what is the protocol for the treatment?
The All India Institute of Medical Sciences (AIIMS) has issued clinical protocol dated April 21, 2020 for treatment of Covid-19 patients and states such as Madhya Pradesh and Delhi have directed Hospitals and health centres dedicated to treating COVID-19 patients to follow the said clinical protocol.[10]
Treatment must be affordable for all. One must know whether or not there is a standardisation of costs of treatment of a COVID-19 for private hospitals?
Government hospitals are reaching their intake capacities and for that reason COVID-19 patients have been resorting to treatment in private hospitals. While some private hospitals are charging exorbitant amounts as costs of treatment, the same is worrying not just for the patients but also to the insurers.[11]
In a first, the State government of Maharashtra has capped treatment costs in private hospitals for people without medical insurance and for other patients, the capped prices will come into effect once they exhaust their medical insurance cover.[12]
The Hon’ble Gujarat High Court has vide its order dated May 22, 2020 directed the state government to issue a notification making it mandatory for all multi-speciality hospitals private/ corporate hospitals in Ahmedabad and on its outskirts to reserve 50% of their beds (or such other capacity as maybe specified by the state government) for COVID-19 patients.
In view of the same, the Government of Gujarat may come up with similar caps on costs as Maharashtra.[13] The Hon’ble Gujarat High Court also observed that the certain private hospitals authorised by the government to treat COVID-19 patients in Ahmedabad are charging exorbitant fees which is unaffordable for a massive section of the society and directed the state government to ensure that private hospitals do not charge exorbitant fees. [14]
Also in light of the same The Hon’ble Bombay High Court recently directed a charitable hospital to make court deposit of monies in a case pertaining to levy of exorbitant charges for treatment of COVID-19 patients belonging to poor strata of the society despite reserving 20% of its beds for poor and the needy.[15]
Corona virus, every day its like we are tuned to the same channel spewing the same things like a factory mill on overwork. But be as it may every day, we learn more about this disease that was thrust suddenly to the world, after initially originating from china. There are many a theory afloat that China deliberately kept the onset of this disease a secret to gain from it, and knowing the level the Chinese usually stoop to it would not be farfetched to believe so. Nearly every country is trying to cope up to this disease with drastic level of differences. On one side we have countries like new Zealand who have virtually negligible cases and still effectively trying to combat the situation and on the other end we have countries like USA where the cases have arisen to such a point that their President has announced that he will be slowing down testing to make it seem like the number of cases have dwindled. So where on this spectrum does India lie?
India is home to a vast population that counts in billions, to safely combat a virus which spreads so easily is a herculean task in itself. However, the front-line workers are continuously working to be the first line of defence, but is it enough. Very often we see on the news and media how heroically our government is fighting the virus, often depicting them as gallant saviours shielding us from the evil virus. The hospitals giving their best in order to help the patients that they get, treating them and sending them back to society so that they may function like before. However, the ground reality is anything but so, with the influx of corona positive cases of nearly 15000 each day, adding the fact that hospitals are seeing the worst mismanagement that could be done during a pandemic, it is no surprise that to many people going to the hospital seems like a walk towards the gallows. The hospitals launched apps in order to increase their efficiency and help them control the crowd gathering in hospitals, however with the traditional Indian scene of mismanagement this has just poured fuel to the increasing fires. The apps show the hospitals having free beds when there are none, mistreating patients and whatnot. Many a hospital within Delhi, India’s capital city have started to look more like morgue, without enough beds to put the dead bodies in, entire floors have been converted into makeshift morgues with bodies simply piled up unhygienically. This is just the tip of the iceberg that is the inefficiency of the hospital scene in battling corona virus. With the amount that an average corona patient is charged, coupled with the gross mismanagement it can make life a living hell for anyone going to the hospital regarding this issue. During this pandemic bed charges have inflated very much, a general ward bed in super specialty hospitals costs around 11000 a day, due to the covid-19 expenses. The overall amount depends on the time period one I admitted. Adding the mismanagement of the hospital staff into the mix it can go for unnecessarily long periods. Counting in the per day costs of a ventilator in the ICU ward for serious cases it can add an additional 50,000 per day as well. Thus, even if one miraculously survives the ordeal of corona, monetarily they are thrust back way harder than before.
What actions we further take is for everyone to see.
Antibacterial Chemotherapy refers to the use of any chemical or drug for the treatment of bacterial diseases. It is the part of antimicrobial chemotherapy. Antimicrobial chemotherapy can be divided into several branches on the basis of type of pathogen, for e.g. For bacterial pathogen – Antibacterial Chemotherapy For viral pathogen – Antiviral Chemotherapy For fungal pathogen – Antifungal Chemotherapy, etc
ANTIMICROBIAL CHEMOTHERAPY – Chemotherapy may either mean involvement of any drug that fight against any cancerous cell or it may involve the use of any antimicrobial drug to cure diseases caused by infectious microorganisms or pathogens. Antimicrobial drugs work by different mechanisms for different type of organisms. The overall mechanism by which any antimicrobial drug functions is by interfering with the structure and/or function of microorganisms. They either directly kill microbial cell or function by inhibiting their growth.
DEVELOPMENT OF ANTIMICROBIAL CHEMOTHERAPY The development of chemotherapy has been known to begin with the successful research of a German physician, Paul Ehrlich (1854-1915). Ehrlich was always fascinated to learn more about the dyes that bind to and stain the microbial cells. He was sure and stated that one of the dyes could be used as a chemical that would selectively destroy or kill the infectious pathogen inside the human body without making any harm to human cell and he named it “Magic Bullet”. Working more on this, he was able to find that the dye, trypsan red was active against the trypanosome that causes African Sleeping Sickness. Later, Ehrlich with his assistant Sahachiro Hata tested a variety of arsenic-based chemicals on Syphilis-infected rabbits and was successful in finding that Arsphenamine (an arsenic based chemical compound) was active against the Syphilis spirochete which was then made available in the market. The other German scientist, Domagk in 1927 found the another Magic Bullet to treat diseases. He observed the antimicrobial activity of a synthetic dye, Prontosil Red which was able to cure Streptococcal and Staphylococcal infections with very limited toxicity. Sulfanilamide (one of the active breakdown products of prontosil in body) was the first synthetic antimicrobial drug.
A Synthetic Antimicrobial is a drug that is developed from any type of a chemical compound that is not found in nature.
Penicillin was the first naturally synthesized antibiotic which was initially discovered by a 21 years old French medical student. No one remembered his work until Alexander Fleming in September 1928 accidently rediscovered the antibiotic. The petri plate of Staphylococcus which was inoculated by Fleming was found to develop certain molds which made the clear zone of inhibition of staph-bacterial species around them. It was meant that the mold infected the petri plates even before the bacteria were inoculated. Fleming suggested that the mold (probably the strain of Penicillium notatum) produced a substance which inhibited the bacterial growth surrounding it and hence had an antibacterial property. Further experiment results concluded that Penicillin was active against streptococci, meningococci and Corynebacterium diphtheriae, which is the causative agent of diphtheria. The isolation, mass production and purification of penicillin were accomplished by Howard Florey and Ernst Chain for which they got the nobel prize. They found that the penicillin once pured was effectively able to show antimicrobial properties against streptococcal infection in mice. Later, Dorothy Hodgkin observed and analyzed the structure of various naturally synthesized products using X-rays. Because of her observation on the chemical structure of naturally synthesized penicillin, it was easier for many scientists to produce a variety of semi synthetic penicillin.
A semisynthetic antimicrobial is defined as the chemically modified product of a natural antibiotic.
After the discovery of penicillin, other scientists got the determination for the discovery of more antibiotics by natural or chemical synthesis. Selman Waksman developed a new antibiotic, Streptomycin which was produced by the actinomycete, Streptomyces griseus. This antibiotic was discovered by the soil microorganisms, particularly bacteria and fungi. It was the first discovery of antibiotic- producing soil microorganism. It was found that streptomycin was successful in treating tuberculosis. Other microorganisms producing chloramphenicol, neomycin, terramycin and tetracycline were also isolated later.







You must be logged in to post a comment.