Nobody was expecting to be one day locked in their homes and worrying about keeping the virus at bay. Untill the vaccines are out we have to take certain serious measures to ensure the safety of our family and loved one’s.
Is cleaning like we usually did enough? What can a common man do without thehigh tech protective gears?
Let us break down some steps which can be followed at home as a part of our daily routines to not only clean but also disinfect :
Food and it’s cleaning procedure:
Nowadays with online shopping of essentials, we must make sure that the vegetables and fruits are disinfected. We must transfer the eatables into a dish and wash off the container immediately. If it is a disposable container, throw it in the trash can which should have a lid. Remove and throw away outer cartons of cereal boxes. All unnecessary shrink wraps and plastic packaging must be disposed off. Beverage bottles and cans can be wiped with disinfectant. Fresh vegetables and fruits must be thoroughly rinsed under a running tap, preferably with warm water and salt and turmeric. Wash your hands with soap and water once you are done. One can also keep certain items in sunlight to naturally kill some germs under the Uv rays.
Washing clothes after returning home:
Warm water destroys germs. So, use the warmest water appropriate for the fabrics you are washing. Use a generous amount of detergent or soap along with disinfectant liquids likke Dettol/ Savlon. Allow the clothes to dry fully, either in the dryer or outside on a clothesline in the sun. All of the above steps are necessary to fully exterminate the virus. Remember to disinfect the laundry bag as well. And wash your hands with soap immediately afterwards.
Disinfect surfaces that are frequently touched:
Surface that are touched very frequently like door knobs, door edges, handrails, light switches, kitchen and living room surfaces, mobile phones, earphones, remote controls, wallets, toilet seats, taps, tables and chairs should be cleaned one a week or even more frequently.
If the surface is too grimy, you first want to clean it with soap and water. Use a clean piece of cloth or a kitchen sponge wipe. Then wipe the surface with a disinfectant wipe or a disinfectant solution that has at least 70% alcohol. You can also use bleach. One cup of bleach mixed with five gallons of water is suitable for non-wood surfaces. For wooden surfaces, a solution of white vinegar and water works well.
The disinfected surface needs to dry naturally. Do not quickly wipe it dry. Most disinfectants need to stay wet on a surface for at least a few minutes in order to be effective. We suggest using a wipeable waterproof cover for your phone. It will be easier to disinfect and there’ll be less chance of the disinfect damaging the device.
Cleaning of floors and walls of theHouse:
Even if you are not using a vacuum cleaner, you can manually sweep and mop the floor with disinfectant. Pay special attention to high-traffic zones like porches, hallways, lobbies, kitchens and corridors. You want to clean the floor in these places more thoroughly. Make this an everyday habit and if you go outside then twice a day is highly recommended.
What to doif you come home from outside:
When you come home from outside, you bring a lot of germs into the house on your clothes, shoes and bags. As soon as you enter the house, remove your shoes and overcoat at the door. Leave your bags in a corner and head straight to the bathroom. Wash your hands, face and other exposed parts with water and soap. Next, disinfect your bags and the things you have brought home. You can use wipes or simply wash them with soap water. You can also sun them out as heat is known to kill coronavirus.
These are some of the few things you can do to make sure you and your family stay safe and healthy through this pandemic.
Biomedical Waste Management & Handling Rules, 1998 (“1998 Rules”) in India govern the handling, disposal and management of bio-medical waste (“BM Waste”)in India have been notified by the Central Government in the exercise of the powers conferred by Section 6,8 & 25 of the Environmental Protection Act, 1986. These rules provide for the framework of the management and Handling of disposal and scientific management of BM Waste
In wake of the COVID-19 pandemic, the Centre Pollution Control Board (“CPCB”) recently issued guidelines dated March 27, 2020 for handling, treatment and safe disposal of BM Waste generated during treatment, diagnosis and quarantine of patients confirmed or suspected to have COVID-19 (“Guidelines”).
The Guidelines have been necessitated due to the super infectious nature of the Novel corona virus and provide for a mechanism for the segregation, packaging, transportation, storage and disposal of BM Waste in order to avoid further spread of the virus through BM Waste.
So what do you mean by the BM Waste and what are the categories of BM Waste that the hospitals generate?
The Bio-Medical Waste Management Rules 2016[1] (“2016 Rules”) define the BM Waste as any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or research activities pertaining thereto or in the production or testing of biological or in health camps, including the categories mentioned in Schedule I the 2016 Rules.
The 2016 Rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form. The next imminent question that comes to our minds is what are the categories of BM Waste that the hospitals generate?
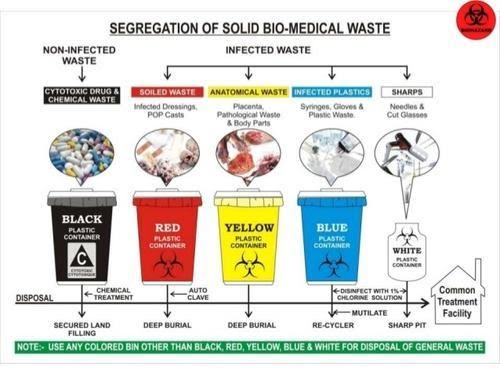
BM Waste generated from a hospital could be human anatomical waste, animal waste- microbiology & biotechnology, waste sharps, discarded medicines and cytotoxic drugs, solid & liquid waste.
Now that we know what’s the meaning and various categories of BM Waste, the most pertinent question arises that how is it supposed to be treated and disposed of by the hospitals in India during the ongoing COVID-19 pandemic?
While the hospitals in their usual course deal with the segregation, management and storage of BM Waste, the situation in times of COVID-19 is extraordinary the reason being the highly contagious nature of the virus and also it’s transmission cycle and multiplicity rate.
As the hospitals are being flooded with the suspected and confirmed cases, the Ministry of Health and family welfare (“MoHFW”) and the CPCB have issued various guidelines for the handling and management of waste generated from the COVID-19 facilities.
Under the 2016 Rules, while the hospitals are required to ensure that there is a secured location within its premises for a spill/pilferage free storage of segregated BM Waste in labelled/coloured bags or containers, the duty to transport the stored BM Waste from the hospital premises onwards to the common BM Waste treatment and disposal facility is of an ‘operator’ as defined in the Rules.
Specifically, in wake of COVID-19, the CPCB has issued Revision 1 to the Guidelines dated March 25, 2020 for Handling, Treatment and Disposal of Waste Generated during Treatment/Diagnosis/ Quarantine of COVID-19 Patients (“CPCB Guidelines”).
[2] The said CPCB Guidelines inter-alia, state that hospitals are required to depute separate BM Waste sanitation workers to COVID-19 isolation wards and maintain records of all waste generated in such isolation wards and ensure that the BWM generated is collected and separately stored in separate leakproof color-coded double layered bags or bins /containers labelled as “COVID-19 waste” as per the 1998 Rules and the Guidelines.
In fact the Bombay High Court in a recent pending public interest litigation has, while issuing notices to local municipal corporations and the State Pollution Control Board, also directed the Maharashtra government to clarify whether it was ensuring that all COVID-19 related biomedical waste generated in the state was being disposed of in a safe manner[3].
Now that we have a thorough understanding of how the BM Waste is supposed to be treated and disposed of the most important and the widely discussed about topic is that what are the measures that a hospital is required to take for the safety of its employees doctors, nurses and other support staff who are known as the (“healthcare personnel”) from the dangerous diseases like COVID-19?
In order to answer this pertinent question which is often there in the limelight, one must keep in mind that the Healthcare personnel who are the Frontline workers have a high risk of contracting the COVID-19.
While the hospitals are taking precautions and measures to control any spread of infection within the premises, it is particularly difficult given the highly super-infectious nature and hyper-speed feature of the virus. Due to this feature it spreads widely and it becomes a bit difficult to contain it in an over-crowded environment but it’s not impossible to achieve that as we all have been deterrent enough to contain it’s spread but still there is always scope for improvement.
The first steps towards controlling the spread of a virus is personal protective equipment also known as PPE which should preferably be a two-layered fluid-resistant apron and basic items like N-95 masks, face shield, full cover gowns and sanitisers but the same are rendered ineffective against the COVID-19 if the quality of these equipments is not up to the standard as required.
Greater emphasis is also to be laid upon the proper training and awareness of healthcare personnel towards proper use and disposal of the equipment. The spread of the COVID-19 virus is also particularly fast due to the heavy load of asymptomatic patients coming into the hospital and hence a greater need for the formulation of national COVID-19 protocol.
The MoHFW has vide its revised guidelines for clinical management of COVID-19 dated March 31, 2020[4] (“Clinical Management Guidelines”) impressed upon strict compliance of Infection prevention control (IPC) protocol for Hospitals and a consequent effect of the same is prevention and management of COVID-19 in the hospital staff.
This protocol inter-alia, standard precautions such as hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin, prevention of needle-stick or sharps injury, safe waste management, cleaning and disinfection of equipment and cleaning of the environment around a COVID-19 patient.
The 2016 Rules also provide as follows that in order to and for ensuring the safety of the healthcare workers and others involved in the segregation and pre-treatment of BM Waste, the hospital is required to train to all its healthcare workers, immunise them for protection against diseases which likely to be transmitted by handling of BM Waste, in the manner as prescribed in the National Immunisation Policy[5].
Also, hospitals are required to ensure occupational safety of all its health care workers and others involved in handling of BM Waste by providing appropriate and adequate PPE and also they must conduct health check ups at the time of induction and at least once in a year maintain the records for the same.
Now due to the pandemic if one is an employee ie the Healthcare personnel of the hospital one must understand the Legal aspect and angle also and the most important aspect of all is that what is the Legal obligations of the hospital, if and when an employee of the hospital tests positive for COVID-19.
Let’s answer this as it’s the most crucial and critical aspect. The present COVID-19 pandemic is an unprecedented event and is unlike any other infectious disease known to mankind and the medical world which is yet to fully decipher its modus operandi of infecting humans.
In a hypothetical situation wherein a hospital employee contracts COVID-19, it will be imperative for the employee in such a situation to establish that his possible exposure to COVID-19 was in the Hospital itself not in the community after considering that the employee is spending time outside as well apart from the hospital premises.
While in an ideal case, if it is proved that a hospital staff has contracted it ,i.e., it shall amount to ‘a hospital acquired infection’, then the hospital would be ordinarily liable. However, in the case of COVID-19 since it is seemingly impossible to trace down the exact source of the infection, in absence of such evidence and in light of utmost safety measures and precautions taken by the hospitals as per the guidelines, fastening of any liability on the hospital would be peculiarly difficult.
The defence available to the hospital may be culpability and negligence of the employee and proving that the hospital itself took all possible measures to avoid any mass spread of the infection.
The next relevant point to be analysed and answered is that when a Non COVID-19 patient contracts the virus during his term of being admitted in the hospital what are the Legal obligations of the hospital when this happens?
The National Consumer Dispute Redressal Commission in the matter of Apollo Emergency Hospital vs Dr. Bommakanti Sai Krishna & Anr.[6] observed that “As already observed, the infection occurred during the stay of the Complainant at the hospital. On the other hand, there is nothing to show that the source of infection lay outside the hospital. Thus, there is preponderance of possibilities of the infection having been acquired in the hospital itself. We therefore, do not accept the contention that it was necessary for the Complainant to produce expert evidence to prove negligence on the part of the concerned doctors in the hospital.”
The afore-stated judgement implies a presumption of liability on the hospital that in cases where the probability of acquiring the infection is much higher inside the hospital than from other sources. However, the same may not apply in COVID cases in light of the peculiar difficulty of tracing the source of acquiring the COVID-19 infection. Therefore, the presumption rendered by the aforesaid judgement will not be ipso facto applicable to cases of COVID patients.
As we have discussed the various pertinent relevant questions another one is that what are the legal obligations of the hospital, if and when a patient is misdiagnosed positive or negative for COVID-19 by the hospital due to a fault in the COVID-19 rapid testing kit (“testing kits”)?
The liability of a hospital in cases of misdiagnosis depends on the methodology of procuring of testing kits. A hospital may procure testing kit either from third party manufacturer or may manufacture them internally i.e. by itself or its subsidiary.
In cases where the misdiagnosis is on account of faulty testing kit procured externally, the hospital cannot be held directly liable as the liability may be shifted upon the manufacturer.
In cases where the misdiagnosis is on account of faulty testing kit is due to testing kits produced internally the hospital may be liable subject to it being proved that the misdiagnosed patient was indeed positive. However, factors such as the success rate of any testing kit not being 100% may have an interplay in determining the liability.
We have to be aware of what are the Legal liability of a hospital in a situation where the hospital discharges a mild/very mild/pre-symptomatic COVID patient to ramp up the capacity for serious COVID-19 patients.
A hospital will not be held liable for a systematic discharge of a mild/very mild/pre-symptomatic/moderate COVID-19 patient as the same is directed by the Central Government. On May 8, 2020, the MoHFW released its revised policy for the discharge of COVID-19 patients.[7] This revised policy provides that hospitals can discharge mild/very mild/pre-symptomatic in accordance with the protocols given therein.
In the earlier advisory[8], COVID-19 patients could be discharged only after chest radiograph clearance, viral clearance in respiratory samples, and if two of the patient’s specimens were negative within a period of 24 hours. The discharged patient would then have to home quarantine themselves in accordance with the revised policy.
So what is the protocol to be followed by a Hospital while disposing of the dead bodies of the COVID-19 patients?
The corpses are a source of infection for healthcare personnel/ other patients and cannot be disposed of by usual methods of disposal and therefore, the MHFW issued guidelines dated March 15, 2020 on dead body management in COVID-19.[9] The guidelines provide inter-alia, the protocol to be followed at the time of removal from the isolation room or area, put in bio-hazard bag and disinfection. Further, all surfaces of the isolation area (floors, bed, railings, side tables, IV stand etc.) should be wiped with 1% Sodium Hypochlorite solution and then it should allow a contact time of 30 minutes, and allow it to air dry as well.
While treating patients infected with the COVID-19 virus, what is the protocol for the treatment?
The All India Institute of Medical Sciences (AIIMS) has issued clinical protocol dated April 21, 2020 for treatment of Covid-19 patients and states such as Madhya Pradesh and Delhi have directed Hospitals and health centres dedicated to treating COVID-19 patients to follow the said clinical protocol.[10]
Treatment must be affordable for all. One must know whether or not there is a standardisation of costs of treatment of a COVID-19 for private hospitals?
Government hospitals are reaching their intake capacities and for that reason COVID-19 patients have been resorting to treatment in private hospitals. While some private hospitals are charging exorbitant amounts as costs of treatment, the same is worrying not just for the patients but also to the insurers.[11]
In a first, the State government of Maharashtra has capped treatment costs in private hospitals for people without medical insurance and for other patients, the capped prices will come into effect once they exhaust their medical insurance cover.[12]
The Hon’ble Gujarat High Court has vide its order dated May 22, 2020 directed the state government to issue a notification making it mandatory for all multi-speciality hospitals private/ corporate hospitals in Ahmedabad and on its outskirts to reserve 50% of their beds (or such other capacity as maybe specified by the state government) for COVID-19 patients.
In view of the same, the Government of Gujarat may come up with similar caps on costs as Maharashtra.[13] The Hon’ble Gujarat High Court also observed that the certain private hospitals authorised by the government to treat COVID-19 patients in Ahmedabad are charging exorbitant fees which is unaffordable for a massive section of the society and directed the state government to ensure that private hospitals do not charge exorbitant fees. [14]
Also in light of the same The Hon’ble Bombay High Court recently directed a charitable hospital to make court deposit of monies in a case pertaining to levy of exorbitant charges for treatment of COVID-19 patients belonging to poor strata of the society despite reserving 20% of its beds for poor and the needy.[15]
Antibacterial Drugs are classified according to their site of action which are as follows :
CELL WALL SYNTHESIS INHIBITORS There are 3 different mechanisms by which anti-cell wall drugs work and thus they are also classified as following:
First classification involves the drugs that directly interact with Penicillin-Binding-Proteins (PBPs) and inhibit the transpeptidase activity which in turn inhibits the attachment of newly formed peptidoglycan subunit to the pre-existing one. This is the main mechanism of β-lactam antibiotics. These antibiotics include Penicillin (penams), cephalosporins, Penems, Carbapenems, and monobactams. These antibiotics bind to the penicillin-binding proteins which are enzymes present in the bacterial cell wall. Different β-lactam antibiotics bind in a different way. After the antibiotics bind to the enzyme, it changes the morphological response of the bacteria to the antibiotic.
Second classification involves the drugs that bind to the peptidoglycan subunit, blocking different processes. The important class of compounds called as glycopeptides are mainly involved in this mechanism of anti-cell wall antibiotics. Vancomycin and Teicoplanin are the major examples of glycopeptide antibiotics. Vancomycin kills only gram-poitive bacteria whereas Teicoplanin is active against both. The overall mode of action of glycopeptides antibiotics is blocking transpeptidation i.e. similar to β-lactam antibiotics, they also inhibit the transpeptidase activity, and transglycosylation i.e. they being large in size attach to the peptidoglycan subunits thus creating a blockage which does not allow the cell wall subunits to attach to the growing peptidoglycan backbone.
Third classification involves the drugs that block the transport of peptidoglycan subunits across cytoplasmic membrane. The main example of such type of drugs is bacitracin, which is a simple peptide antibiotic originally isolated from Bacillus subtilis. The mode of action of these class of drugs is blocking the activity of specific cell membrane lipid carriers which act as the attachment surface for peptidoglycan precursors and help in their movement from cell cytoplasm to exterior of the cell. This activity of lipid carriers is inhibited by bacitracin like drugs and they finally prevent the incoroporation of those precursors into cell wall thus inhibiting its biosynthesis.
Although, its route of administration is mostly oral or intramuscular, bacitracin is also known to show its effects when used as topical ointments like Neosporin.
INHIBITORS OF PROTEIN SYNTHESIS Protein Inhibitors can be divided into 2 parts:
Inhibitors binding to 30S subunits • Aminoglycosides bind to the bacterial ribosome, after which they cause tRNA mismatching and thus protein mistranslation. This occurs by mismatching between codons and anticodons, which synthesize proteins with incorrect amino acid. This mistranslated protein, along with correctly translated proteins move into move into the periplasm where most of the mistranslated proteins are degraded and some of them are inserted into cytoplasmic membrane. This causes disruption of the membrane, ultimately killing the bacterial cells. • Tetracyclines are bacteriostatic and block the binding of tRNAs with the ribosome during translation thus inhibiting protein synthesis. Most of the tetracycline class of drugs are broad spectrum and are active against wide range of bacteria.
Inhibitors binding to the 50S subunit • Macrolides are the large class of naturally produced secondary antibiotics. They are basically broad spectrum, bacteriostatic antibiotics. Their main mode of action is blocking peptide chain elongation and they inhibit the formation of peptide bond. Patients allergic to penicillins are recommended erythromycin which is a macrolide. • Lincosamides include lincomycin and clindamycin. Though they are structurally different but functionally similar to macrolides. They are specifically known to inhibit streptococcal and staphylococcal infections. • Chloramphenicol also inhibits peptidyl transferase reaction inhibiting peptide bond formation. It was the first broad spectrum antibiotic and is very much active against a broad range of bacterial pathogens but is very toxic and can cause side.
INHIBITORS OF MEMBRANE FUNCTION Biological cytoplasmic membranes are basically composed of lipids, proteins and lipoproteins. The cytoplasmic membrane acts as a selective barrier which allows the transport of materials between inside the cell and the environment. A number of antibacterial agents work by targeting the bacterial cell membrane. They basically are involved in the disorganization of the membrane. Polymyxins and Lipopeptides are the main anti- cell membrane agents.
NUCLEIC ACID SYNTHESIS INHIBITORS These drugs inhibit nucleic acid synthesis function by either of the following:
Interfere with RNA of bacterial cell Antibacterial drugs of this mechanism are selective against bacterial pathogenic cells. For example: The drug rifampin, belonging to the drug class rifamycin blocks the bacterial RNA polymerase activity. It is also active against Mycobacterium tuberculosis and thus id used in the treatment of tuberculosis infection. It also shows side effects.
Interfere with DNA of bacterial cell There are some antibacterial agents that interfere with the activity of DNA gyrase. The drug class fluoroquinolones show this mechanism. They are borad spectrum antibacterial agents. Some examples of drugs in fluoroquinolone family are Ciprofloxacin, Ofloxacin, Moxifloxacin, etc
INHIBITORS OF METABOLIC PATHWAYS There are some antibacterial drugs which act as ANTIMETABOLITES and inhibits the metabolic pathways of bacteria. • The sulfonamides block the production of dihydrofolic acid. This blocks the production of purines and pyrimidines required for nucleic acid synthesis by blocking the biosynthesis of folic acid. Their mechanism of action is bacteriostatic and they are broad spectrum antibacterial agents. Though humans also obtain folic acid but these drugs are selective against bacteria. Sulfones are also structurally and functionally similar to sulfonamides. • Trimethoprim is used in the same folic acid synthesis pathway but at a different phase, in the production of tetrahydrofolic acid. • There is another drug, Isoniazid which is an antimetabolite only selective against mycobacteria. It can also be used to treat tuberculosis when used in combination with rifampin and streptomycin.
INHIBITORS OF ATP SYNTHASE There is a class of drug compounds called as Diarylquinolones that are specifically active against mycobacterial growth. They block the oxidative phosphorylation process and finally leading to reduced ATP production which either kill or inhibit the growth of mycobacterial species.
Choosing an antibacterial drug therapy can depend on various factors which are mentioned below:
BACTERIOSTATIC V/S BACTERICIDAL Antibacterial chemotherapeutic agents can be categorized as bacteriostatic and bactericidal on the basis of their interaction with the targeted bacterial pathogens. Bacteriostatic drugs work by inhibiting the growth of specific bacteria. Static drugs work by reversibly inhibiting the growth i.e. if the agent (drug) is removed or if its effect if over, the microorganism will get recovered and will grow again causing the same infection again. Bactericidal drugs work by directly killing the target bacteria from the location. Cidal drugs may act as static drugs at low concenteration.
Use of any drug also depends on the immune system of the host because static drug does not completely eliminate the target bacteria. For patients with strong immune system, either static or cidal drugs can be used for curing infection while in case of immunocompromised individual, only cidal drugs are essentially required for complete removal of the bacterial infections.
SPECTRUM OF ACTIVITY On the basis of their range or spectrum of activity, the chemotherapeutic agents can be broadly categorized into 5 different categories:
Narrow spectrum antibiotics are only active against less no. of microorganisms. They target only a specific strains of bacterial pathogens, especially gram positive bacteria.
Moderate spectrum antibiotics target most of the gram positive bacterial pathogens as well as most systemic, enteric and urinary tract gram negative bacterial pathogens.
Narrow and moderate spectrum antibiotics are known to cover all the β-lactam antibiotics which can effectively work against gram positive and negative bacteria. Some members of this classification are only effective against gram negative while others can also kill gram positive bacteria.
Broad spectrum antibiotics, as the name suggests targets a broad range of bacterial pathogens which includes almost all the prokaryotic organisms except mycobacteria and pseudomonas. They are also effective against polymicrobic infections (mixed infections caused by multiple bacterial species). It is used when other spectrum antibiotics fail to treat infections due to drug resistance. There is a risk of superinfection while using broad spectrum antibiotics.
Anti-mycobacterial antibiotics are only effective against mycobacterial strains of pathogenic bacteria.
DOSAGE AND ROUTE OF ADMINISTRATION • Dosage – The minimum or maximum amount of drug that a patient is given is the dosage of the drug. The dosage of the particular drug needs to be determined carefully to ensure that the optimum level of that particular drug is achieved at the site of infection for the elimination of the infection without causing any toxic side effects. Therefore, the selection and standardization of dosage of a particular drug is done so that it has the minimum side effect. • Route of administration – It can be defined as the method by which a drug is introduced in the patient’s body. There are different ways of administration of a drug. The most preferred drugs are the one that can be administered orally because it is easier for the patients to take them even at their home without visiting the health care professionals again and again. However, it is observed that not all drugs can be absorbed from the gastro intestinal tract. E.g. Bacitracin, Polymyxin and many antifungals. These drugs may be available to the patients in the form of topical preparations so that they can be applied for the treatment of superficial skin infections. The another condition arises when a patient is unable to take oral drug initially due to some illness like vomiting. In that condition, the drug is preferably administered through parenteral route i.e. intramuscular or intravenous injections. In general, for most of the drugs, the drug levels in plasma introduced via intravenous is higher than that of oral or intramuscular route.
POTENTIAL FOR SIDE EFFECTS The adverse effects which are seen in the patient’s body after administration of any drug can be classified into 3 main types:
PHARMACOLOGICAL SIDE EFFECTS These are the toxic side effects which the drug shows by damaging the infected or even healthy cells by the production of some toxic chemicals on cell surface or their interior.
ALLERGIC SIDE EFFECTS Some drugs show the allergic reactions in the patient’s body which is due to the antigen-antibody reaction which in turn effects other cells and show some allergy.
BIOLOGICAL TYPE SIDE EFFECTS This type of side effect is worst and it involves interference of the drug with the normal microflora of the body which is followed by either local chemical damage or superinfection.
POTENTIAL INTERACTION BETWEEN DRUGS Most of the time, antibiotics are administered in the patient’s body as a single agent but many time it becomes necessary to take two or more drugs at a time. So, different drugs administered at a single time show some interaction among them. The interaction may be positive or negative. Sometimes, a synergistic or positive interaction is shown by two antibiotics when they are administered together. Some drugs show bactiostatic effect when used as a single agent but are able to show bactericidal effect when combined with other antibiotic. On the other hand, some drugs when used together show negative effect or antagonistic effect. Antagonism can occur between two antimicrobial or between one antimicrobial and one non-antimicrobial. The antagonistic interactions thus cause toxic side effects, loss of drug activity, decreased effect of drug at the site of infection. For e.g. Penicillin and bacteriostatic drugs are antagonists of each other.
The pandemic of Coronavirus that has engulfed the globe has also motivated us to find solutions for living life with Coronavirus. Our life will not be the same as it was till Coronavirus is around and the medical fraternity comes up with certain medicine that would increase the chances of survival of the people. A nationwide debate has begun about the reopening of schools and educational institutions.
The lock down that commenced from March did not affect the academics as the majority of learning was already completed and only assessment was to be completed. Students could stay at home safely during the spread of the Coronavirus due to the timely closure of the educational institutes by the government.
The time has come when the new academic year is about to commence. The government and the educational stakeholders are in a fix over the methodology or concrete path to be followed for the reopening of the schools. What should be the guidelines to obviate the fear of all the stakeholders about economical aspects and above all safety of students.
The medical perspective has put forth two issues one is safety and protection of the students, teachers, and families, and the other is the prevention of the spread of disease through schools as a hub for the same. Students have a habit of socializing and they are at greater risk than those who will follow the medical guidelines in letter and spirit. It is a difficult task to ensure all the youngsters at schools and colleges following the guidelines on keeping themselves safe. India is a densely populated country and the cases of Corona infection are on rising day by day. Hence, a judicious and careful approach for the reopening of the schools is considered by the government by finding a novel approach to handle the situation.
Factually the corona infected cases are increasing in India and experts have been forecasting that the country may reach a peak in July. Keeping in view the aspect of the increase in the number of corona viruses infected patients by July would pose a different challenge to the government if it opens the schools. Parents association and some activists have already filed cases in the court of law for seeking a delay in the opening of schools.
Though in urban areas online classes are about to become a routine concept. The condition of rural areas in terms of online connectivity is a matter of concern, putting the rural students at a disadvantage. A thought over long term impact on students residing in remote areas and with no resources be also given.
The students can be called to school physically in the second half of the academic year, in the first half certain measures that would reduce the burden on students and the teachers can be initiated. Reduction in the syllabus is one such aspect. The planned conduct of online classes can help all to achieve concrete success in the first half.
The development of a vaccine is in progress and let us hope that we get the same soon. This is the time when we can redefine the education system and help the Education sector find a new beginning. We need to provide the best education to the students.




You must be logged in to post a comment.